This publication has been updated, please see here for the latest version.
According to several recent Guttmacher Institute analyses, the Affordable Care Act (ACA) is clearly working to increase insurance coverage for women of reproductive age, with substantial declines in the percentage who are uninsured. However, the studies also make clear that not all groups of women are benefiting equally from the ACA, and that Latinas and immigrant women are more likely than other women to remain uninsured.
As previous Guttmacher calculations of health insurance coverage have shown, Medicaid and private insurance coverage increased considerably between 2013 and 2014, the first full year of ACA implementation. These findings are echoed in and bolstered further by two new Guttmacher analyses:
- The first, recently published in Contraception, analyzes details about health insurance coverage among women aged 18–39, using survey data from 2012 and 2015 collected by the Guttmacher Institute.
- Results of the second analysis, which are presented below, track changes in insurance coverage between 2013 and 2014 among women aged 15–44 using data from the U.S. government’s American Community Survey (ACS), which is particularly well-suited for state-level analysis and complements similar previous analyses.
Among the key takeaways from this body of work are the following points:
Less Insurance "Churn": The study from Contraception found that women spent less time uninsured after the ACA than before: Greater numbers of women reported uninterrupted coverage in 2015, and those reporting a gap in coverage in the last six months were more likely to be uninsured for only one month. As the authors note, "Reducing this ‘churn’ promotes continuity of care and helps women afford care—including often time-sensitive reproductive health care—when they need it."
Unequal Progress for Latinas and Immigrant Women: Despite the substantial improvements in health insurance coverage among women overall, it is lagging for certain groups, including Latinas and immigrant women. According to the Contraception study, U.S.-born Latinas had twice the odds of being uninsured as white women; foreign-born Latinas had more than four times the odds.
The ACS analysis found that significant coverage gaps remain among immigrant women who are not citizens (see graphic below). In 2014, the first full year of the ACA’s implementation, immigrant women who were not U.S. citizens were more than three times as likely to be uninsured as women born in the United States (42% vs. 13%). Those differences were even greater for the subset of those women living at or below the federal poverty level (57% of noncitizen women were uninsured vs. 22% of U.S.-born women).

Furthermore, although many immigrant women gained coverage between 2013 and 2014, the proportion of women who were uninsured fell by only 10% (from 47% to 42%) among noncitizen immigrant women compared with a drop of 22% (from 17% to 13%) among U.S.-born women. The trends for noncitizen women indicate that policy and legal barriers to public and private insurance options are continuing to bar millions of immigrant women and their families from affordable coverage and care.
Significant Variations by State: Another key finding of the research is that the improvements in insurance coverage are tied to the ACA’s coverage expansions—and specifically to the major expansion to Medicaid now adopted by 31 states and the District of Columbia. In the Contraception study, women who lived in a non-expansion state had twice the odds of being uninsured as women who lived in a state that had expanded Medicaid.
A previous Guttmacher analysis found that states that implemented the ACA’s Medicaid expansion for 2014 experienced both steeper declines and lower overall levels in their uninsured rate among women of reproductive age: Only 11% of women were uninsured in expansion states, but 18% were in non-expansion states. Additionally, while Medicaid expansion states already had higher levels of Medicaid coverage prior to the ACA, that gap grew in 2014: Some 23% of reproductive-age women in expansion states had Medicaid coverage compared with 17% of reproductive-age women in non-expansion states.
The ACS analysis found particularly large improvements in coverage in states that had expanded Medicaid. For example, Kentucky and West Virginia saw the largest decreases in uninsurance (declines of 10 percentage points each, representing 44–45% fewer women uninsured), driven by increases in Medicaid enrollment. Both of these states expanded Medicaid eligibility under the ACA, though the newly elected governor of Kentucky is seeking to roll back his state’s expansion.
Additional state-level trends in women’s coverage from the ACS analysis include:
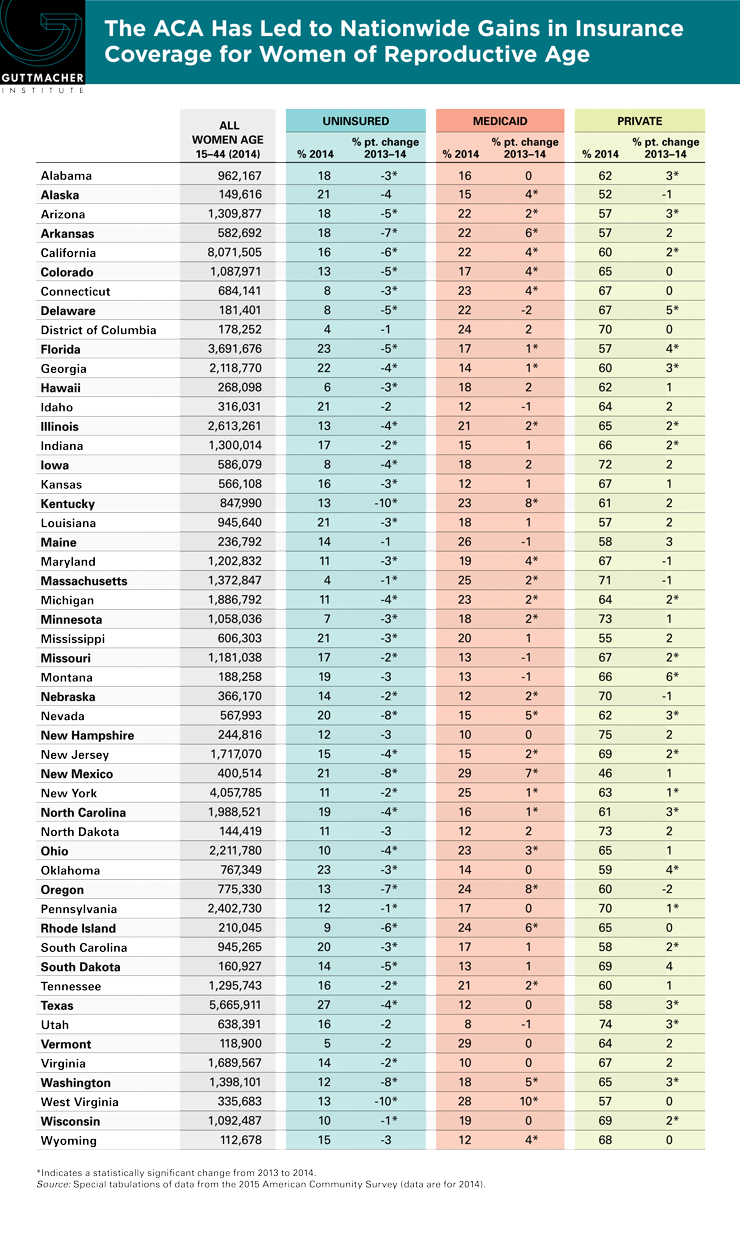
- From 2013 to 2014, the percentage of uninsured women of reproductive age decreased in every state and the District of Columbia; this change was statistically significant in 41 states. Whether these declines were driven by increases in public or private coverage, or both, varied by state (see table).
- Twenty-seven states (most of which expanded Medicaid under the ACA) had significant increases in the proportion of women covered by Medicaid. Kentucky, Nevada, Oregon, West Virginia and Wyoming had the greatest growth in women covered under Medicaid, representing at least 50% more women covered in 2014.
- Twenty-two states had significant increases in the proportion of women covered by private insurance; however, these increases were more modest than the changes for Medicaid. Montana and Delaware had the greatest growth in women with private coverage, representing 10% more women with private coverage in 2014.
- In 2014, Texas had the greatest proportion of women (27%) who still had neither public nor private coverage, while only 4% of women in Massachusetts and the District of Columbia remained uninsured.
In summary, the ACA has advanced coverage among U.S. women of reproductive age, with significant implications for women’s access to health care generally, and sexual and reproductive health services specifically.