Key Points
- Modern contraceptive services and maternal and newborn health care are essential for protecting the health of Pakistani women, their families and communities.
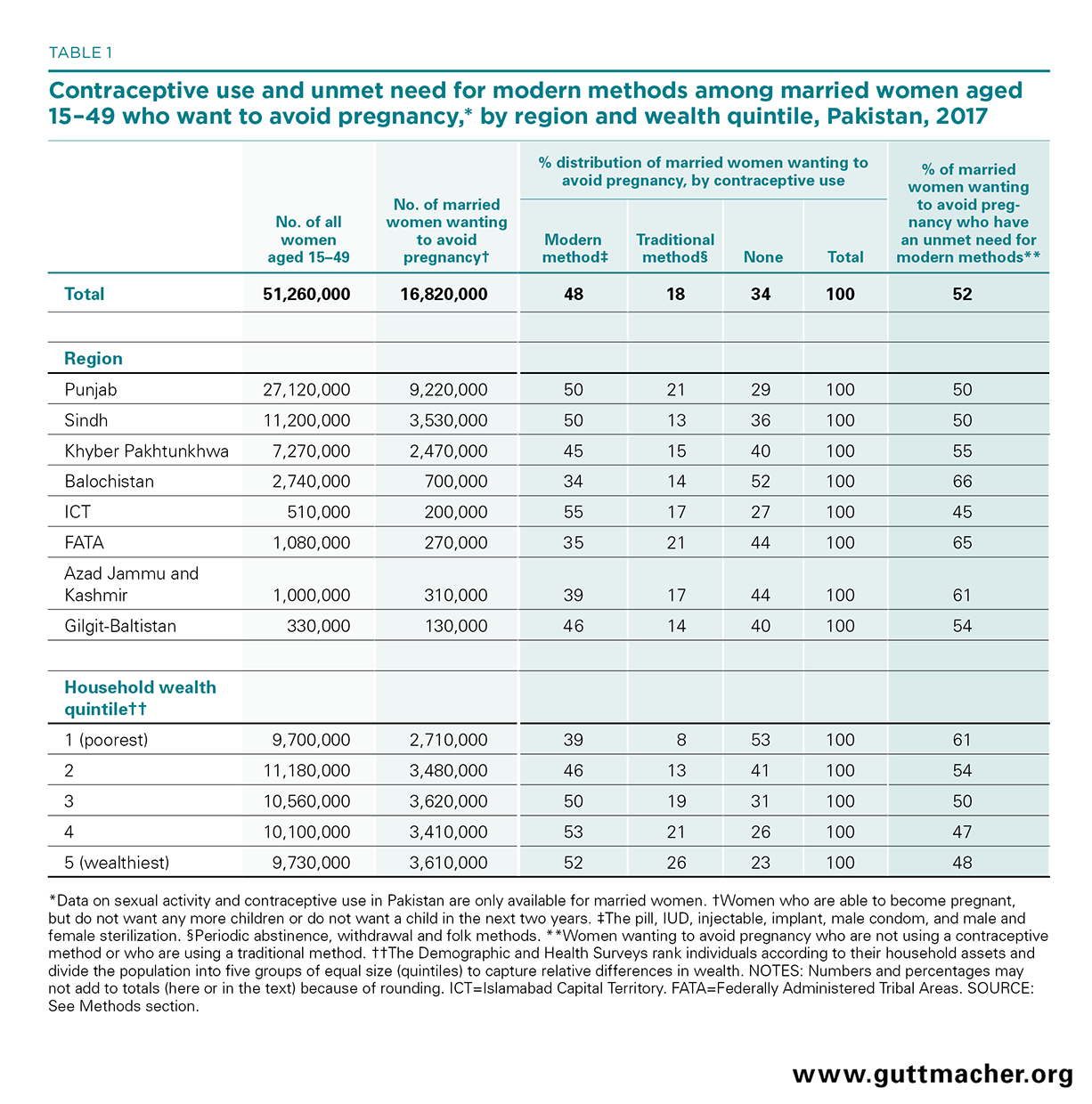
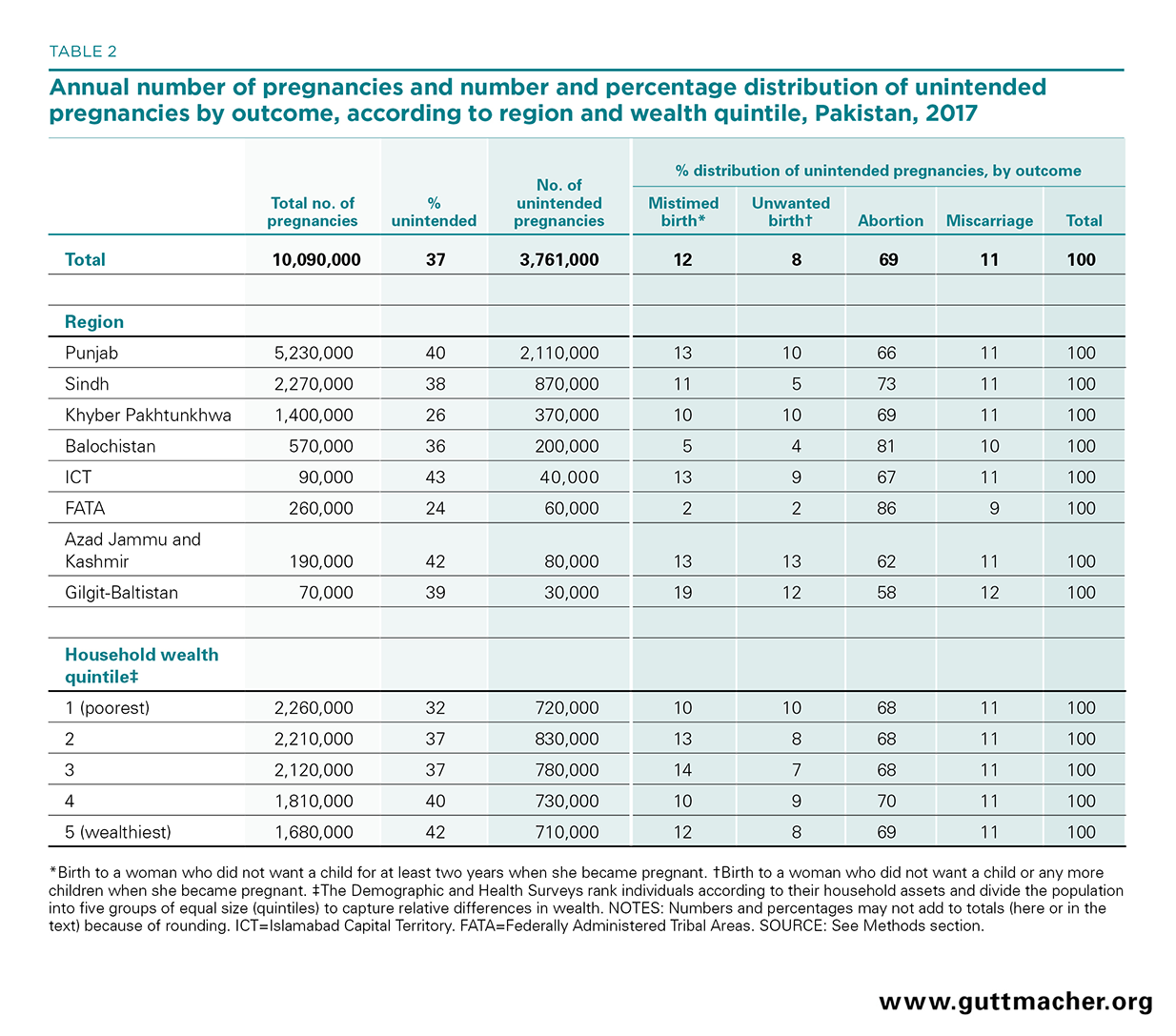
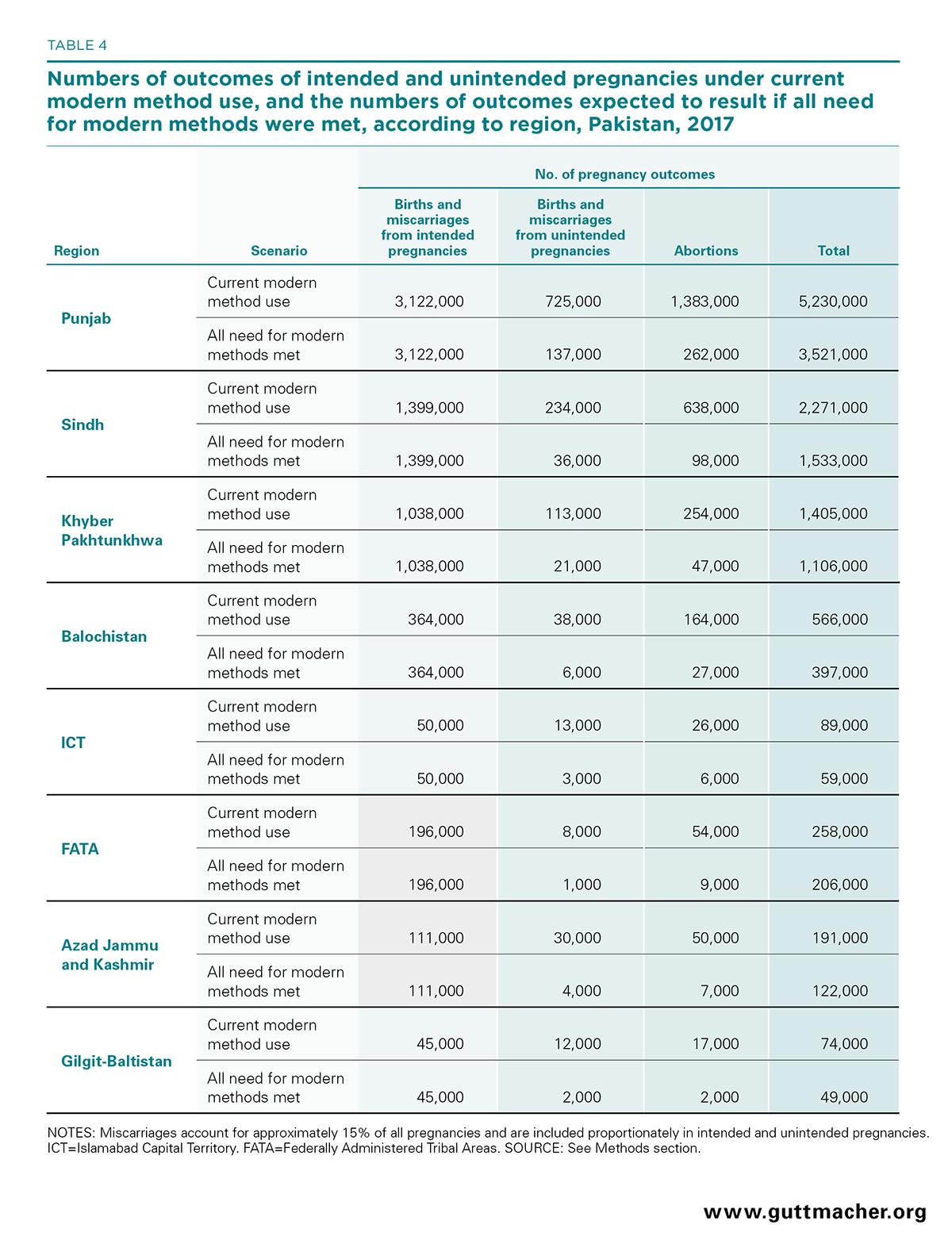
- Based on data from 2017, women in Pakistan have an estimated 3.8 million unintended pregnancies each year, most of which result from unmet need for modern contraception.
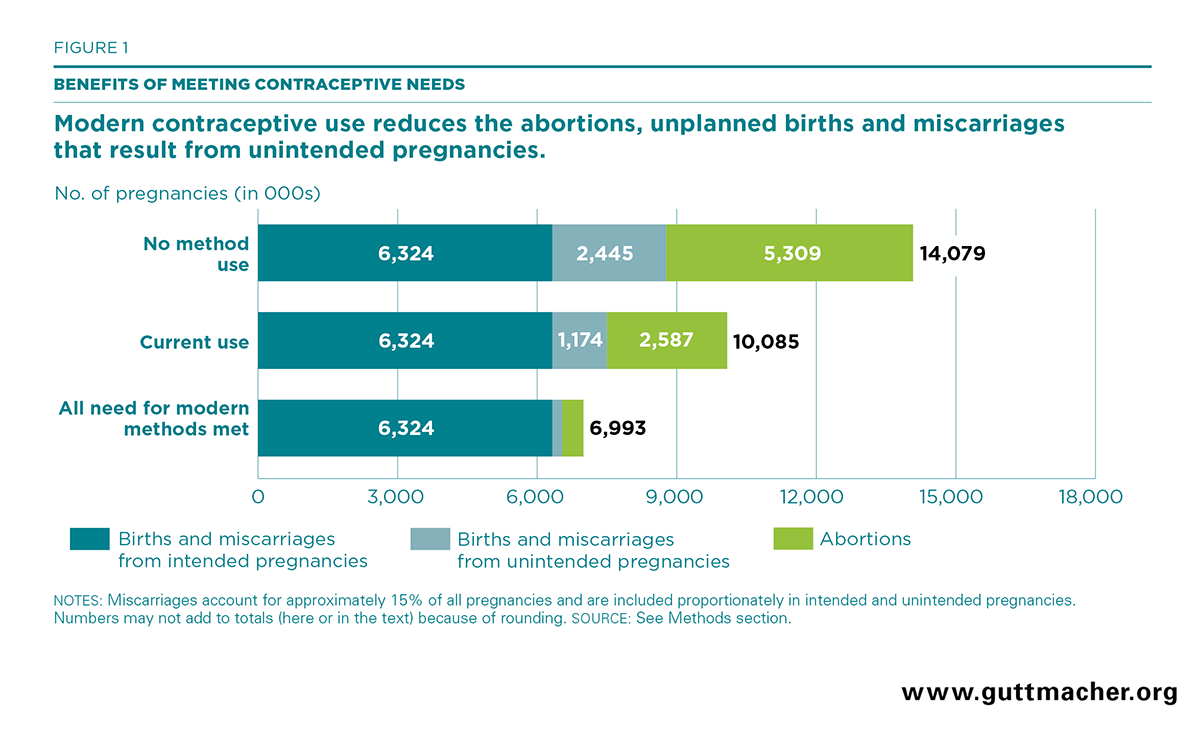
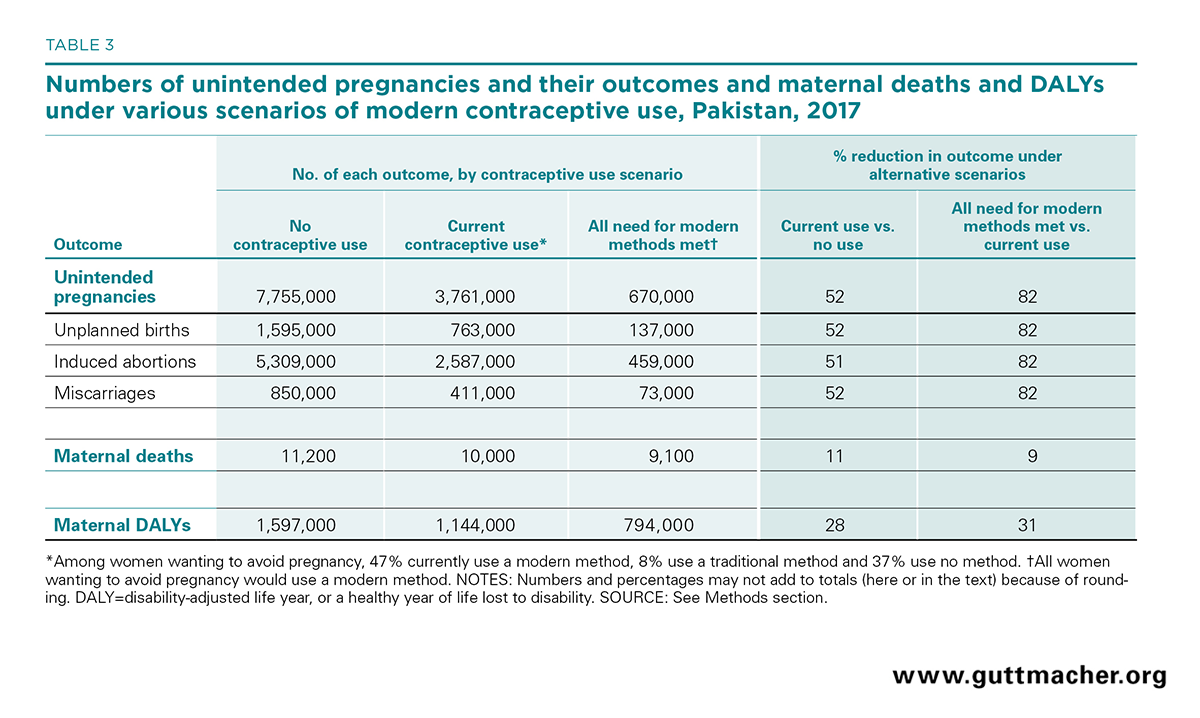
- About 52% of married women of reproductive age (15–49) who want to avoid a pregnancy are not using a modern contraceptive method. If all unmet need for modern contraception were met, there would be 3.1 million fewer unintended pregnancies annually, 2.1 million fewer induced abortions and nearly 1,000 fewer maternal deaths.
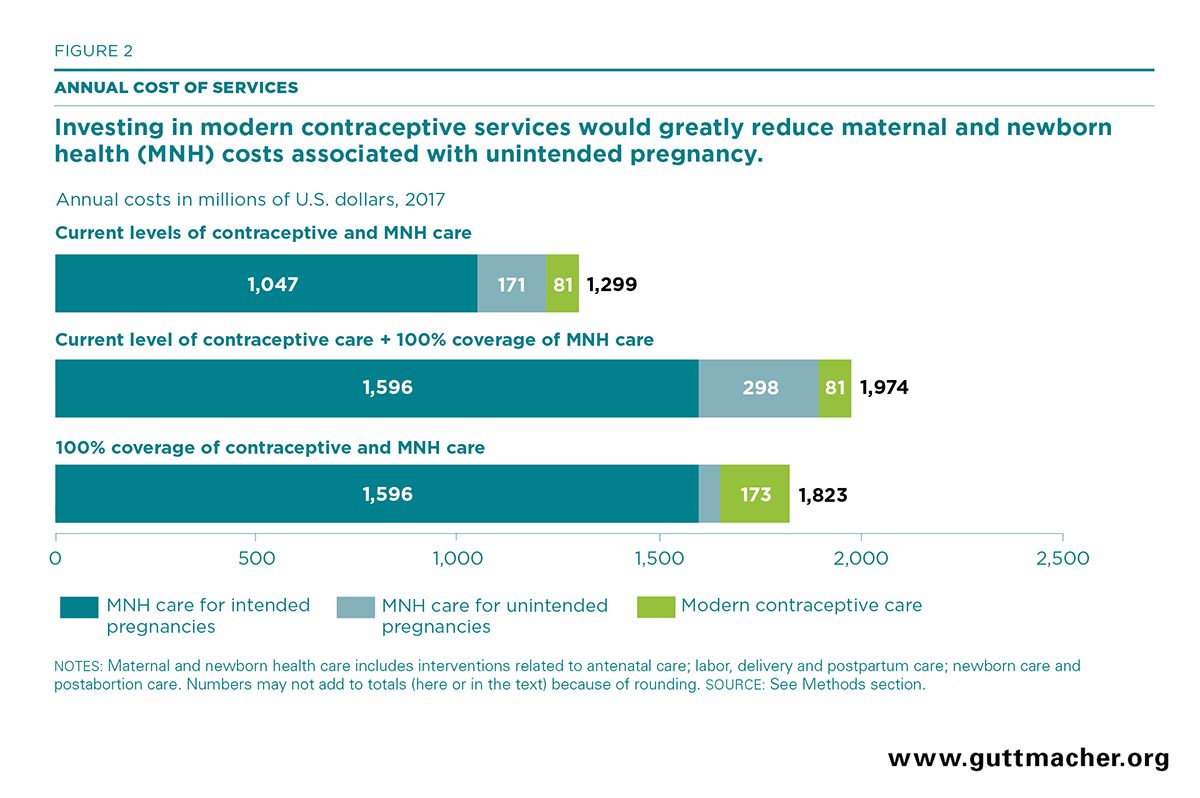
- Pakistan is currently spending US$81 million per year on contraceptive services. Serving the full unmet need for modern contraception would require an additional US$92 million per year, for a total of US$173 million, based on public-sector health care costs.
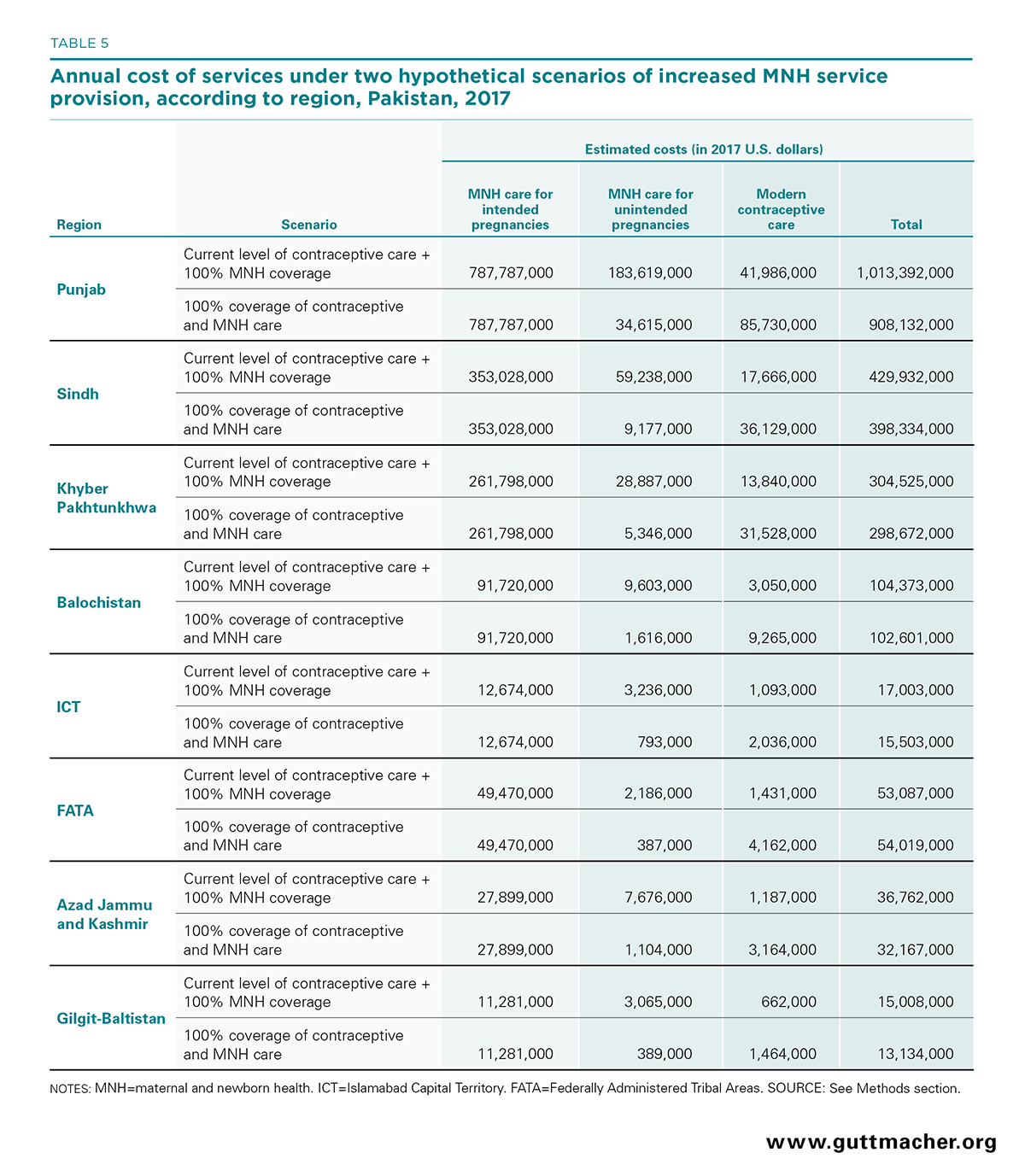
- At current levels of contraceptive use, providing maternal and newborn health care to all women who have unintended pregnancies, at the standards recommended by the World Health Organization, would cost an estimated US$298 million.
- If all women wanting to avoid a pregnancy used modern contraceptives and all pregnant women and their newborns received the recommended care, the country would save US$152 million, compared with a scenario in which only maternal and newborn health care were increased. Punjab would see the largest savings (US$109 million).
- The combined investments would be cost-effective: For every additional dollar spent on expanding modern contraceptive use, the country would save more than US$2.50 on maternal and newborn care.
- Provincial governments, the federal government, the private sector and international development partners must all increase their investment in modern contraceptive services to fully meet the need for modern contraception.