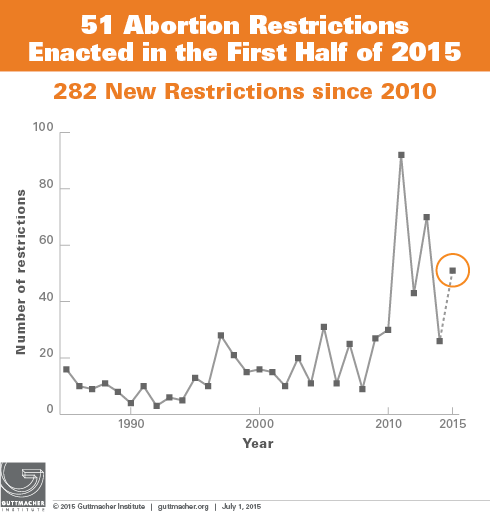
So far this year, states have enacted 51 new abortion restrictions; this brings the number of restrictions enacted since 2010 to 282. Although only about a dozen states remain in session as of July 1, these states may well enact additional restrictions before the end of the year. Following the recent pattern of increased restrictions in odd-numbered years (largely because not all legislatures are in session in even-numbered years), states have enacted more restrictions during the first half of this year than during all of last year (see chart). But nonetheless, the number of new restrictions this year is well below the 70 enacted in 2013, due in part to fewer restrictions being enacted in a handful of states—including Kansas, Oklahoma and Arizona—that had adopted multiple restrictions between 2011 and 2014.
Even as states continue to pass new abortion restrictions, the Supreme Court is poised to hear one, and maybe two, major abortion cases in the coming year. The Court might take a case challenging a 2013 Texas law that requires abortion providers to have admitting privileges at a local hospital and imposes Targeted Regulation of Abortion Providers (TRAP) requirements on abortion clinics in the state. The U.S. Court of Appeals for the Fifth Circuit upheld the law in May. In June, the Supreme Court granted a request for an emergency stay, blocking enforcement of the provisions. Abortion rights supporters are widely expected to file a full appeal to the Supreme Court in the coming months (see The State of Sexual and Reproductive Health and Rights in the State of Texas: A Cautionary Tale). In addition, the Court is weighing whether or not to hear a case in the fall centering on Mississippi’s law requiring abortion providers to have hospital admitting privileges.
Although states have adopted a wide range of restrictions so far this year, much of the attention has focused on four areas: waiting periods, abortions after the first trimester, medication abortion and TRAP provisions. Even though most action on these issues follows recent trends, some states have charted some new directions that may well serve as models for other states going forward.
Waiting Periods
Three states moved this year to extend the length of their existing waiting periods, and two additional states adopted new waiting periods. Arkansas and Tennessee mandated a 48-hour wait between counseling and the abortion procedure. North Carolina and Oklahoma enacted measures requiring women to wait at least 72 hours, joining Missouri, South Dakota and Utah, which also require women to wait at least three full days for an abortion (see Counseling and Waiting Periods for Abortion). A new Florida law, which would establish a 24 hour waiting period, has been challenged and it remains to be seen if enforcement of the law will be blocked during the court case.
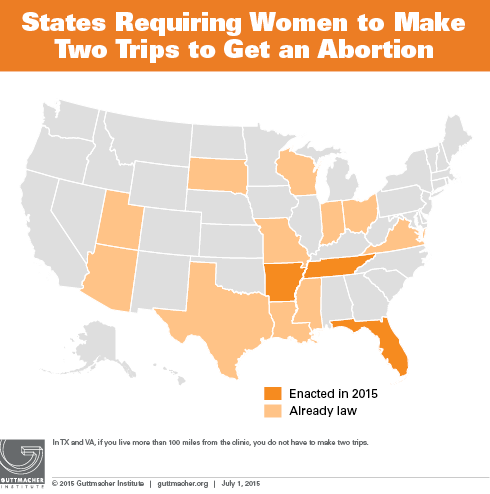
Significantly, three of the five states to adopt waiting period requirements this year also require women to receive abortion counseling at the abortion facility, effectively necessitating two trips. Making multiple trips exacts a high toll on women, many of whom have to travel, often at considerable expense, to obtain the care they need (see A Surge of State Abortion Restrictions Puts Providers—and the Women They Serve—in the Crosshairs). In June, the new “two trip” requirement in Florida was challenged. Although this law went into effect on July 1, opponents have asked that it be blocked as the legal proceedings continue; a decision on that request could happen at any time. Including Florida, as well as Arkansas and Tennessee, the two other states with new legislation this year, 14 states require women to make two trips to obtain an abortion (see map).
Abortion Restrictions After the First Trimester
Since 2010, 14 states have adopted measures banning abortion at about 20 weeks postfertilization (about 22 weeks after the woman’s last menstrual period) and 11 of these states have laws in effect. This includes a new law in West Virginia, which was enacted when the legislature overrode Gov. Earl Ray Tomblin’s (D) veto (see State Policies on Later Abortions).
For the first time, two states, Kansas and Oklahoma, enacted measures that could ban abortion as early as 14 weeks of pregnancy. These new laws use nonmedical, vague and inflammatory language to try to ban abortion procedures commonly used in the second trimester. The Kansas law was challenged in early June on the grounds that it violates the state’s constitution by infringing on a woman’s ability to access a safe abortion method and dictating medical practice; the law is not in effect pending resolution of the challenge. Similar measures are likely to be proposed in other states.
Medication Abortion
Including three that enacted measures this year to limit access to medication abortion, 19 states now restrict this commonly used first-trimester abortion method (see Medication Abortion).
- Banning telemedicine. Although telemedicine is increasingly used to expand access to health care in underserved areas, states have moved aggressively in recent years to ban its use for medication abortion. This year, Arkansas and Idaho adopted new restrictions, join 16 other states in barring this use of telemedicine. In mid-June, the Iowa State Supreme Court struck down a regulation banning the use of telemedicine for medication abortion, saying that no evidence supported the imposition of such an undue burden on women; the regulation had not been in effect pending the court decision.
- Requiring FDA protocol. Arkansas enacted a measure requiring use of the outdated protocol that appears on the FDA label for mifepristone that was approved in 2000. The newer evidence-based regimen uses less medication, involves fewer side-effects and visits to the provider and is less expensive; this new regimen is routinely used and is widely recognized as the standard of care for performing medication abortion. Including Arkansas, four states nonetheless require use of the outdated FDA protocol.
- Counseling on reversing medication abortion. Arizona and Arkansas adopted a new type of medication abortion restriction: Under these laws, abortion providers are required to inform women that it is possible to stop a medication abortion by giving the woman a large dose of hormones after the mifepristone has been administered, but before the woman takes the misoprostol. However, very little evidence indicates that this works to stop the abortion procedure or that it does not entail medical risks. The Arizona law has been challenged in federal court and is not being enforced.
Targeted Regulation of Abortion Providers (TRAP)
Four states enacted measures that impose restrictions on abortion providers beyond what is necessary to ensure patients’ safety. Typically, these laws take two approaches: establishing physical plant and staffing standards, and requiring abortion providers to have a formal relationship with a hospital (see TRAP Laws Gain Political Traction While Abortion Clinics—and the Women They Serve—Pay the Price). Including the new measures enacted this year, 25 states have some form of TRAP law (see Targeted Regulation of Abortion Providers).
- Admitting privileges. Five states require providers of either medication or surgical abortion services to have admitting privileges at a local hospital. Another 10 require the provider to have either admitting privileges or another type of relationship with a hospital (such as an agreement with a physician who has privileges). This year, Arkansas adopted a new restriction that requires only medication abortion providers to have an agreement with a physician who has admitting privileges; the law does not include a parallel requirement for surgical abortion providers. Arkansas is the only state to have such a requirement. Continuing its longstanding effort to require abortion providers to have a relationship with a hospital, the state adopted a new law that requires proof of such a relationship as a condition of obtaining a license to operate in the state.
- Physical plant standards. Legislation adopted by Tennessee in May would require surgical abortion facilities to meet all the requirements for licensure as an ambulatory surgical center; implementation of the law is blocked pending resolution of a legal challenge. Twenty-two states impose standards on abortion providers that are comparable to those for ambulatory surgical centers.
- Disposal of fetal remains. Arkansas and Indiana now require abortion providers to either incinerate or bury fetal remains.