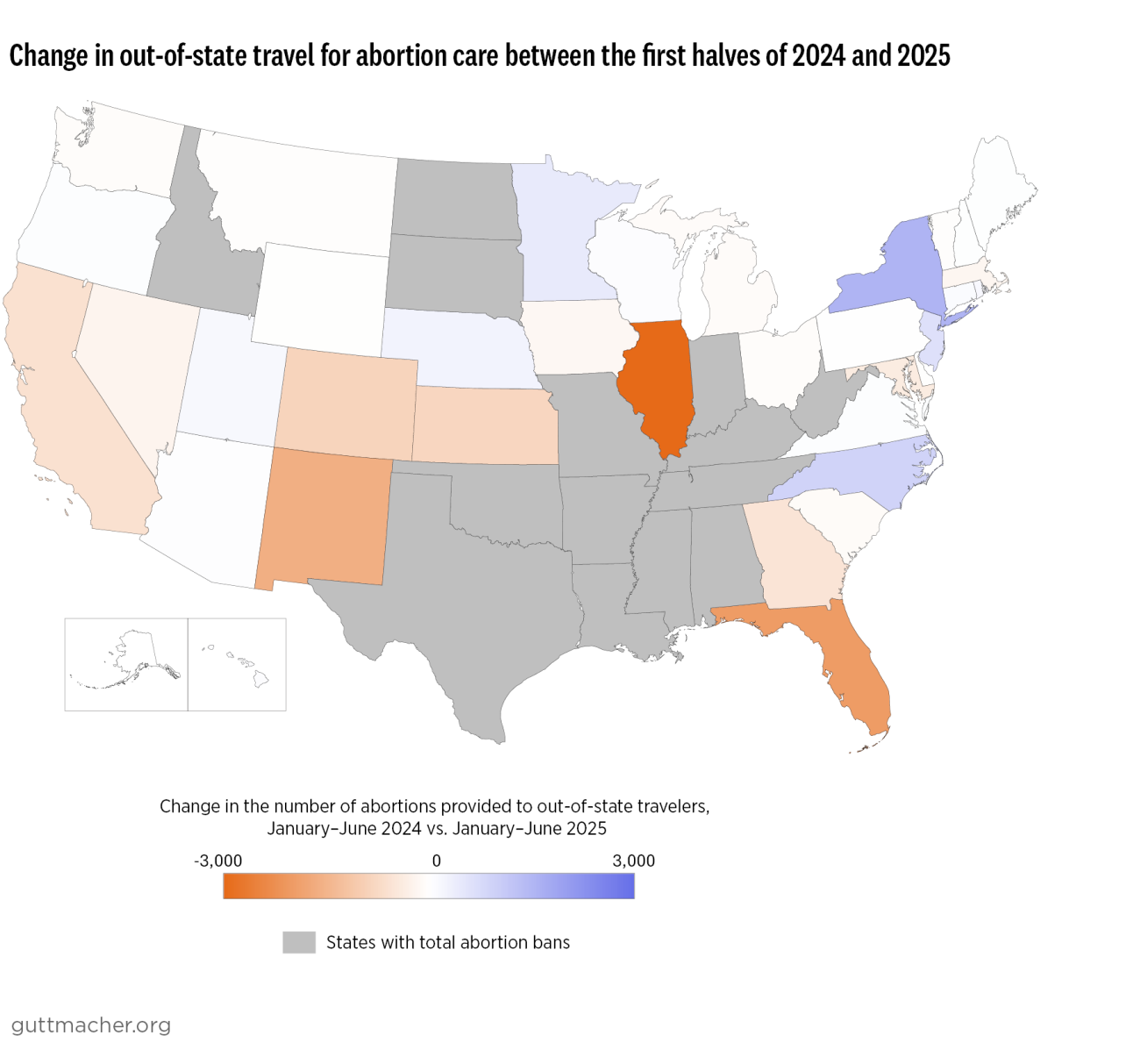
In Illinois, abortion provision declined by 9% between the first halves of 2024 and 2025—with 71% of this decline due to a decrease in the number of patients who traveled to Illinois during this period and the remainder due to declines among Illinois residents. In New Mexico, declines in out-of-state travel accounted for all of the 15% decline in caseloads observed between the first halves of 2024 and 2025. Kansas and Colorado—other major destinations for out-of-state patients—also saw declines in out-of-state travel during this period.
Still, out-of-state travel for abortion care remains significantly higher than pre-Dobbs levels and creating a welcoming policy and provision climate for people traveling for care should continue to be a priority for governors, state attorneys general, state legislators, advocates and clinicians. Importantly, some states saw increases in the number of out-of-state patients between the first halves of 2024 and 2025. In New York, for example, out-of-state travel increased by 51% during this period, likely due to an increase in people traveling from Florida. Taking into account our findings for all states without total bans, however, travel for abortion care appears to be on the decline, likely due to a number of factors.
Shield laws are likely contributing to these changes
Eight abortion-protective states have enacted shield laws that provide legal protections for clinicians to prescribe and mail abortion pills directly to patients in states with total abortion bans or telehealth restrictions, offering these patients a critical point of access despite their states’ extremist policies. Consequently, online clinics offering abortion care to individuals in ban states are expanding.
While shield law provision may not be an appropriate or preferred option for some patients—those at later gestational durations, for example, or those who prefer procedural abortion to medication abortion—this critical innovation is likely a key factor in reducing travel for abortion care, particularly by residents of states with total bans. As the Monthly Abortion Provision Study only captures abortions occurring in states without total abortion bans, it is possible that increasing shield law provision to states with total bans could partially account for the declines in overall caseloads and travel between the first halves of 2024 and 2025. Nationally, the #WeCount project estimates that 40,890 abortions were provided under shield laws to states with total bans in the second half of 2024, up from 35,250 in the first half of the year.
Logistical and financial barriers to travel may also be driving this shift
Travel across state lines can come at a significant cost for patients, who must factor in transportation, lodging, childcare, time off work, and a variety of other expenses, in addition to the cost of the abortion itself. Some patients may also consider increased risks of travel related to rising ICE activity and anti-immigrant hostility. The intensive efforts of clinicians, abortion funds and practical support organizations (as well as patients themselves) have been key in facilitating interstate travel for abortion. However, this work may not be sustainable; abortion funds in ban states like Texas as well as protective states like New York are reporting decreased donations while costs for abortion and related services are rising, potentially reducing support for out-of-state travelers.
Options for travel, meanwhile, are increasingly constricted for many residents of states with total bans. In the first half of 2024, over 3,000 individuals traveled to Florida for abortion care; in the first half of 2025, with the six-week ban in place, just 1,130 did so. Virginia is now one of two states in the Southeast that allows abortion beyond six weeks, and the only one with no forced waiting period. As a result, residents of the region may be increasingly reluctant to travel, as there are few nearby options for care. Those who cannot travel, and do not obtain care via shield law provision, may be self-managing their abortions or be forced to remain pregnant.
The Data Point to Critical Policy Interventions
This early look at the 2025 abortion provision landscape sheds light on how changing factors are impacting abortion access—and how policymakers and advocates can support patients despite the anti-abortion climate of many states and the threats to abortion access posed by the Trump administration.
Shield law protections have expanded care options for people in ban states, and it is of little surprise that such laws are a key target of the anti-abortion movement. From litigation to legislation, conservative lawyers and policymakers are weaponizing the legal system in an attempt to eliminate this critical modality of care. More states should pass shield laws with explicit protections for telehealth provision and policymakers should continue to analyze the provision landscape to evaluate and strengthen existing shield law protections. States should also follow Colorado, Massachusetts, Maine, New York, Vermont and Washington in allowing shield law providers’ names to be removed from prescription labels and replaced with the names of their health care facilities to protect sensitive data, along with considering other data privacy protections.
In addition to enacting shield laws, policymakers can address the financial burdens imposed on patients traveling out of state for abortion care. States and cities can fund abortions directly and should also evaluate these financial assistance programs to ensure efficient and timely access for patients. States can also consider following Maryland’s innovative use of unspent Affordable Care Act surcharge savings to supplement abortion funds.
Tracking state-level abortion provision is critical to analyzing the impacts of changing abortion policies and offering a roadmap for lawmakers everywhere to protect access to essential health care. While everyone deserves access to abortion when, where and how they desire it, the reality is that hostile policy climates and financial and logistical barriers prevent many people from getting the abortion care they seek. These new data from the Monthly Abortion Provision Study, indicating a reversal of recent trends in abortion provision, can thus offer critical new insights into how state policies and abortion funding networks impact patients’ ability to access care.
Methodology
Data are drawn from Guttmacher’s Monthly Abortion Provision Study, which produces estimates of the number of abortions provided by clinicians in states without total abortion bans based on data collected from samples of abortion providers. Estimates include abortions provided at brick-and-mortar facilities (including those that use telehealth) and online-only providers (including providers who mail abortion pills to patients in states without total bans under the protection of shield laws). These estimates do not include self-managed abortions or any abortions involving medication mailed to states with total abortion bans (either self-managed or provided by out-of-state clinicians).