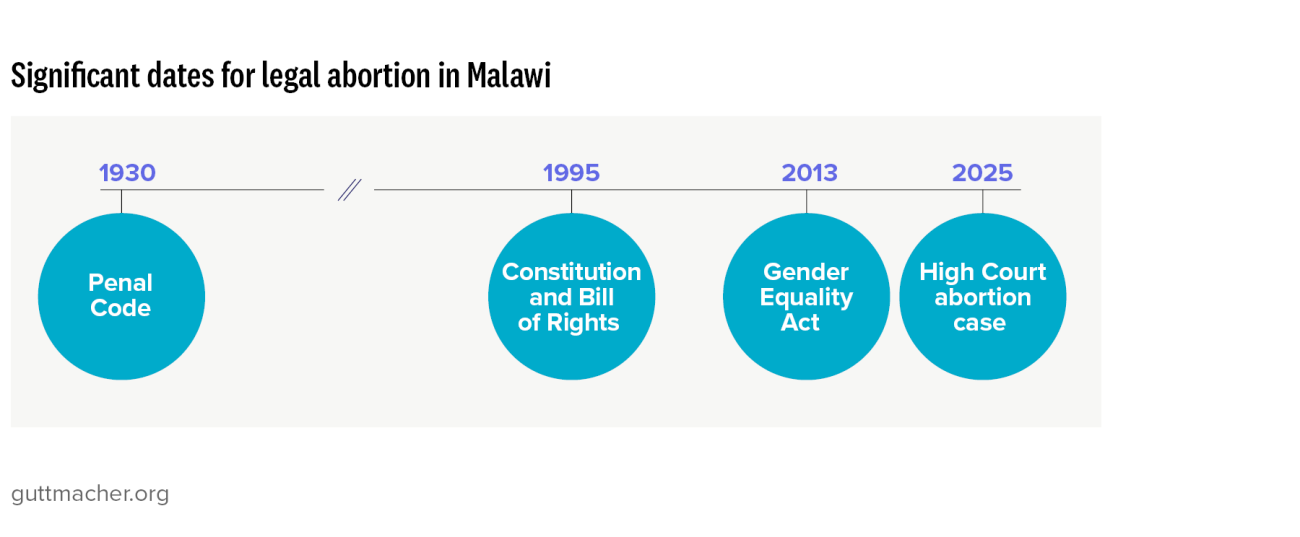
1. Malawi Penal Code (1930), Chapters XIV–XXII, Articles 149–151 and 243.
2. High Court of Malawi, AC (A Minor) v. Solomon and Others, MWHCCiv 14, Oct. 28, 2025, https://malawilii.org/akn/mw/judgment/mwhcciv/2025/14/eng@2025-10-28.
3. Malawi Ministry of Health, Standards and Guidelines for Comprehensive Abortion Care, 2020, https://abortion-policies.srhr.org/documents/countries/10-Malawi-Standa….
4. Chikhwaza O, Evaluation of the Implementation of the 2020–2025 Post Abortion Care (PAC) Standards and Guidelines in Malawi Report, unpublished report, 2025.
5. Malawi Ministry of Health, special tabulations of data on 2024 abortion complication cases.
6. Polis CB et al., Incidence of induced abortion in Malawi, 2015, PLOS One, 2017, 12(4):e0173639, https://doi.org/10.1371/journal.pone.0173639.
7. Bearak J et al., Country-specific estimates of unintended pregnancy and abortion incidence: a global comparative analysis of levels in 2015–2019, BMJ Global Health, 2022, 7(3), https://doi.org/10.1136/bmjgh-2021-007151.
8. Guttmacher Institute, Malawi country profile, 2025, https://www.guttmacher.org/regions/africa/malawi.
9. Mhango P et al., “I am carrying a baby whose father I do not know”: experiences and context of girls pregnant from rape and sought sexual and reproductive health services, 2024, https://doi.org/10.21203/rs.3.rs-5322790/v1 (preprint).
10. Coast E et al., Adolescent abortion care trajectories and safety in Ethiopia, Malawi, and Zambia: a comparative mixed methods study, PLOS Global Public Health, 2025, 5(5):e0004469, https://doi.org/10.1371/journal.pgph.0004469.
11. Riches J, Jafali J and Lissauer D, Report on the Confidential Enquiry into Maternal Deaths in Malawi: August 2020–December 2022, Malawi Ministry of Health, 2022, https://www.mlw.mw/wp-content/uploads/2024/05/Confidential-Enquiry-into….
12. World Health Organization (WHO), Trends in Maternal Mortality Estimates 2000 to 2023: Estimates by WHO, UNICEF, UNFPA, World Bank Group and UNDESA/Population Division, Geneva: WHO, 2025, https://www.who.int/publications/i/item/9789240108462.
13. Mgawadere F et al., Factors associated with maternal mortality in Malawi: application of the three delays model, BMC Pregnancy and Childbirth, 2017, 17(1):219, https://doi.org/10.1186/s12884-017-1406-5.
14. National Statistical Office (NSO), Utica International and ICF, Malawi Demographic and Health Survey 2024: Final Report, Zomba, Malawi: NSO; Columbia, MD, USA: Utica International; and Rockville, MD, USA: ICF, 2025.
15. Geubbels E, Epidemiology of maternal mortality in Malawi, Malawi Medical Journal, 2006, 18(4):208–228, https://doi.org/10.4314/mmj.v18i4.10923.
16. Gondwe MJ et al., Ending preventable maternal deaths in Malawi: the stakeholders consensus approach to identify maternal health needs priorities, BMC Health Services Research, 2025, 25:357, https://doi.org/10.1186/s12913-025-12468-4.
17. Chakhame BM et al., Effectiveness of a training intervention in increasing the use of misoprostol in postabortion care in Malawi: a quasi-experimental study, BMJ Open, 2022, 12:e061886, https://doi.org/10.1136/bmjopen-2022-061886.
18. Wagenheim CA et al., Health care providers’ perceptions of using misoprostol in the treatment of incomplete abortion in Malawi, BMC Health Services Research, 2022, 22(1):1471, https://doi.org/10.1186/s12913-022-08878-3.
19. Chakhame BM et al., Women’s perceptions of and experiences with the use of misoprostol for treatment of incomplete abortion in central Malawi: a mixed methods study, Reproductive Health, 2023, 20(1):26, https://doi.org/10.1186/s12978-022-01549-w.
20. Grossman A et al., Availability of medical abortion medicines in eight countries: a descriptive analysis of key findings and opportunities, Reproductive Health, 2023, 20(1):58, https://doi.org/10.1186/s12978-023-01574-3.
21. Miller C, Maternal mortality from induced abortion in Malawi: What does the latest evidence suggest?, International Journal of Environmental Research and Public Health, 2021, 18(19):10506, https://doi.org/10.3390/ijerph181910506.
22. Miller C, Legalisation of abortion and maternal mortality in Ethiopia, Ethiopian Medical Journal, 2022, 60(2), https://emjema.org/index.php/EMJ/article/view/1855.
23. Miller C, Does legalising abortion reduce deaths from unsafe abortion? Experiences in Sub-Saharan Africa, in: Tingle J et al., ed., Research Handbook on Patient Safety and the Law, Northampton, MA, USA: Edward Elgar Publishing, 2023, pp. 108–124, https://www.elgaronline.com/edcollchap/book/9781802207064/chapter8.xml.
24. Morgan LM and Wendland CL, Debunking misinformation about abortion-related maternal mortality in Africa, Global Public Health, 2025, 20(1):2499915, https://doi.org/10.1080/17441692.2025.2499915.
25. Amoah Twum MA, Govender R and Asunka J, Africans Strongly Support Women’s Autonomy in Marriage and Reproductive Decisions, but Are Divided on Contraceptive Access, Afrobarometer, Dispatch No. 1080, 2025, https://www.afrobarometer.org/publication/ad1080-africans-strongly-supp….
26. Masina, Lameck, Malawi Parliament rejects debate on liberalizing abortion law, Voice of America, March 12, 2021, https://www.voanews.com/a/africa_malawi-parliament-rejects-debate-liber….
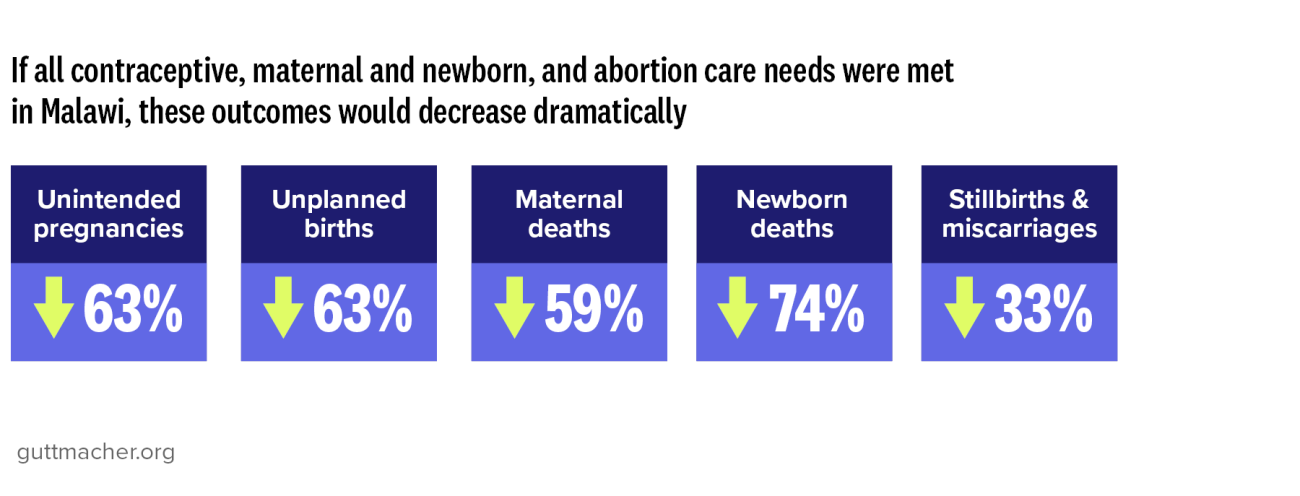
27. Sully EA et al., Adding It Up 2024: Investing in Sexual and Reproductive Health in Low- and Middle-Income Countries, New York: Guttmacher Institute, 2025, https://www.guttmacher.org/report/adding-it-up-2024-investing-sexual-and-reproductive-health-low-and-middle-income-countries.