New findings from the Monthly Abortion Provision Study show that an estimated 1,026,690 abortions occurred in the formal health care system in 2023, the first full calendar year after the US Supreme Court’s decision in Dobbs v. Jackson Women's Health Organization overturned Roe v. Wade. This represents a rate of 15.7 abortions per 1,000 women of reproductive age,* and is a 10% increase since 2020, the last year for which comprehensive estimates are available. It is also the highest number and rate measured in the United States in over a decade.
This increase demonstrates that people continue to seek and obtain abortion care despite the drastic reduction in abortion access in many states. Since the Dobbs decision, in 2022, 14 states have banned abortion with limited exceptions. In addition, seven states—Arizona, Florida, Georgia, Nebraska, North Carolina, South Carolina and Utah—have implemented laws that restrict abortion access on the basis of gestational duration. While access has decreased dramatically in states with bans, almost all other states have experienced substantial increases in the number of abortions provided. As a result, the United States continues to face a fractured abortion landscape, with access varying widely based on where people live and what resources they have.
It is important to note that these annual estimates are almost certainly an undercount, as they include only those abortions obtained within the formal US health care system: at brick-and-mortar health facilities, such as clinics or doctor’s offices, and via telehealth and virtual providers.
Abortion Numbers Are at Their Highest in More Than a Decade
Guttmacher has been tracking the number of abortions in the United States since 1973. Over that time, there have been large changes in abortion incidence in response to changes in access to and demand for abortion care.
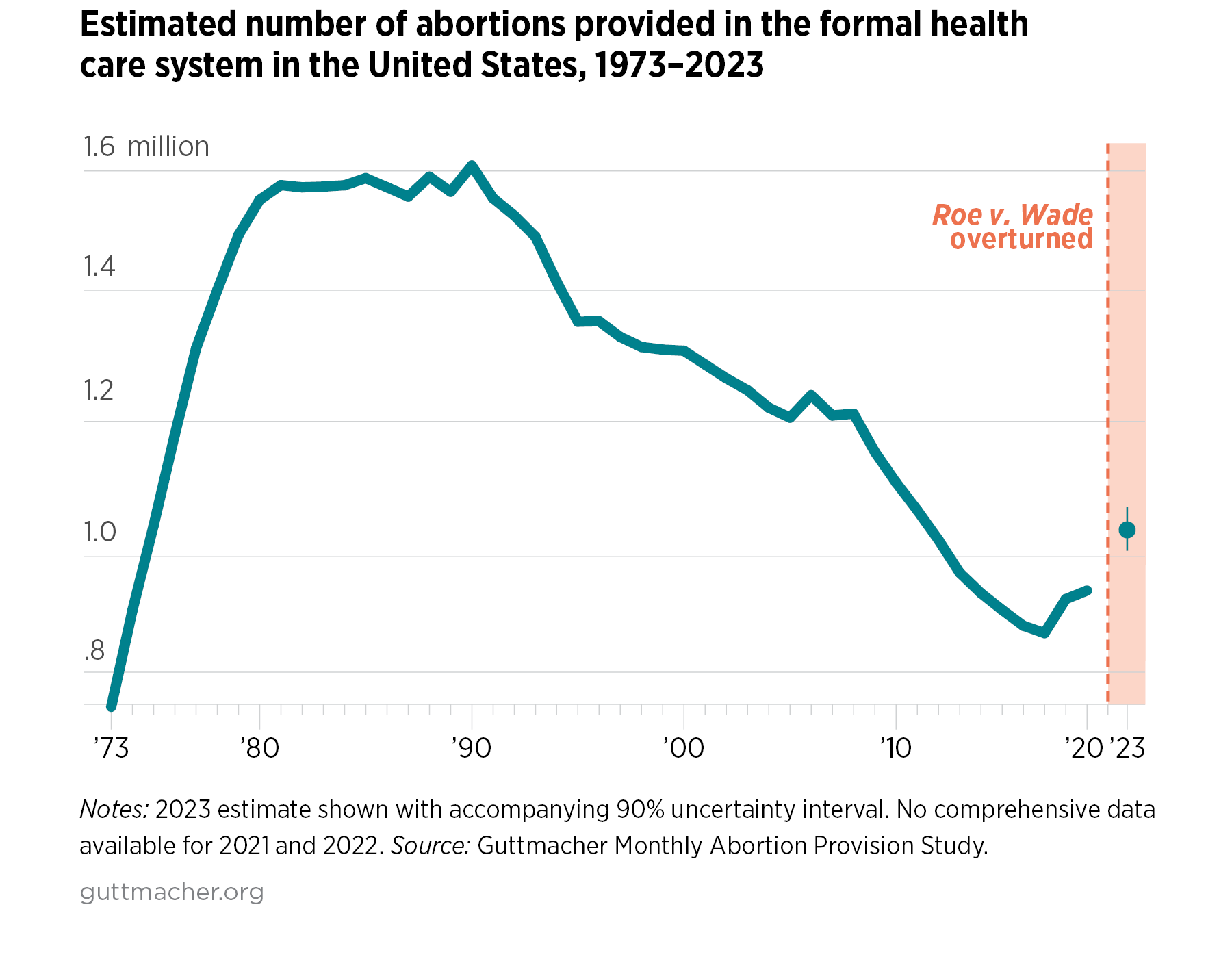
The number of abortions in the United States peaked in 1990, at 1.6 million. Over nearly 30 years, they experienced a sustained decline, falling to 885,000 in 2017. In 2019 and 2020, however, this long-term trend started to reverse, with the number of abortions rising to 930,160 in 2020, marking an 8% increase from 2017 (see Additional Downloads for appendix table). While there are no comprehensive estimates for the next several years, partial data from the Centers for Disease Control and Prevention suggest that this increase continued at least into 2021.
Our estimated 2023 numbers represent a substantial increase even in this historical context; the last time there were over a million abortions provided in the formal health care system in the United States was in 2012.
Why Has Abortion Increased?
Increases in the number of abortions were close to universal—almost every state without a total ban saw an increase in the number of abortions provided, as compared to 2020.†
The 10% increase at the national level in many ways understates the degree to which health systems, providers and support networks have had to scale up care. This is because it does not speak to the large shifts in where people are able to obtain abortions: states without total bans experienced a 25% increase in abortions provided in 2023, as compared to 2020.
In part, this is because the drastic loss of access in states with bans has been counterbalanced by monumental efforts on the part of clinics, abortion funds and logistical support organizations to help people in ban states access care through financial and practical support. States bordering ban states had particularly large increases.‡ In total, abortions in these states increased by 37% between 2020 and 2023, with particularly sharp increases in Illinois (38,010 more abortions than in 2020, or an increase of 72%), New Mexico (15,090 more abortions, an increase of 257%), Virginia (14,190, an increase of 76%) and North Carolina (12,970, or 41%). Much of the increase in these states was due to increased travel across state lines. Illinois, for example, provided abortion care to an estimated 25,660 more patients from out of state, accounting for 68% of its overall increase.
Not all increases at the state level can be attributed to increased travel across state lines, however. Even states not bordering ban states saw large increases—in total, abortion numbers increased in these states by 17%§ from 2020 to 2023. It is very possible that, while access was dramatically curtailed for people living in ban states, access substantially improved for residents of states without bans. Several factors potentially contribute to this increased access:
- Broader availability of telehealth for medication abortion. The use of telehealth to provide medication abortion via mail increased considerably after the U.S. Food and Drug Administration lifted in-person dispensing requirements of mifepristone—one of the drugs most commonly used in medication abortion—during the pandemic. Telehealth now represents a substantial portion of abortion provision in states without abortion bans. Numerous providers, including virtual clinics, have adapted telehealth to meet patient needs, and the availability of telehealth may have increased access, particularly for people in rural areas or who otherwise may not have been able to travel to a clinic for care.
- Increased financial support. Cost has always been an obstacle for people seeking care. The average cost of an abortion was $550 in 2017, and in states where abortion is not covered by Medicaid, the vast majority of patients pay out of pocket. Increased financial support post-Dobbs—particularly from abortion funds—was a critical source of funding for people in ban states and may have increased access for many people living in states without bans as well. It is unclear, however, whether this financial support will be sustainable over time. The National Network of Abortion Funds recently reported that funds across their network reported a large increase in donations post-Dobbs, but those donations have dramatically slowed while the need for assistance has only increased.
- State policies improving protections and access to care. Twenty-two states and Washington, DC have “shield laws” that protect health care providers—and, in some instances, volunteers and patients—from legal or professional consequences enforced by states banning abortion. Some states explicitly protect providers who prescribe and send medication abortion to patients in ban states; note that our data does not include this kind of provision to states with total bans in our counts. Other states enacted policies to protect patient access, to support the health care workforce through grants and financial support, to expand data privacy for recipients of sexual and reproductive health care services or to increase funds for clinic security.
Increases in abortion numbers can be positive if it means that more people are accessing needed care. They can also reflect larger shifts in people’s childbearing desires over time. Changes in people’s desires regarding when and whether they want to have children can play a major role in increases or decreases in abortion incidence. Though some research has suggested there were at least short-term changes in childbearing desires during the COVID pandemic, there have been limited data on changes in childbearing desires post-Dobbs.
Increases Do Not Negate the Impact of Anti-Abortion Policies
This increase in abortions does not diminish the impact of Dobbs on people’s lives. Instead, the data provide important evidence that people will continue to seek abortion care in spite of the policy barriers that anti-abortion policymakers impose. We know now that over 160,000 patients traveled out of state in 2023 to seek abortion care. Individuals traveling across state borders must overcome significant economic and logistical barriers. We also know that many others were unable to obtain care in the formal health care system, and some were forced to continue their pregnancies.
Communities of color, LGBTQ+ people, young people, immigrants, people living with low incomes and those living with disabilities already contend with multiple barriers to accessing care. Anti-abortion policies exacerbate the health inequities these communities face. For example, states with abortion restrictions on the books have fewer maternal care providers and higher maternal death rates, both of which especially harm Black and Brown people. Policy solutions must center the lived experience of those who are disproportionately affected by the fall of Roe. Policymakers should follow the leadership of these communities as they create policies to mitigate the harm of the abortion crisis.
State policymakers must develop and pass robust laws that support people’s ability to access abortion care with dignity and respect—for their own residents and for patients from other states. Federal policies, such as the Abortion Justice Act and the Women’s Health Protection Act, should be enacted. Creative policy solutions at every level of government are needed to ensure that all people can access the care they need regardless of where they live.