
Legislators Have Introduced 445 Provisions to Restrict Abortion So Far This Year
So far this year, legislators have introduced 1,256 provisions relating to sexual and reproductive health and rights. However, states have also enacted 22 measures this year designed to expand access to reproductive health services or protect reproductive rights.

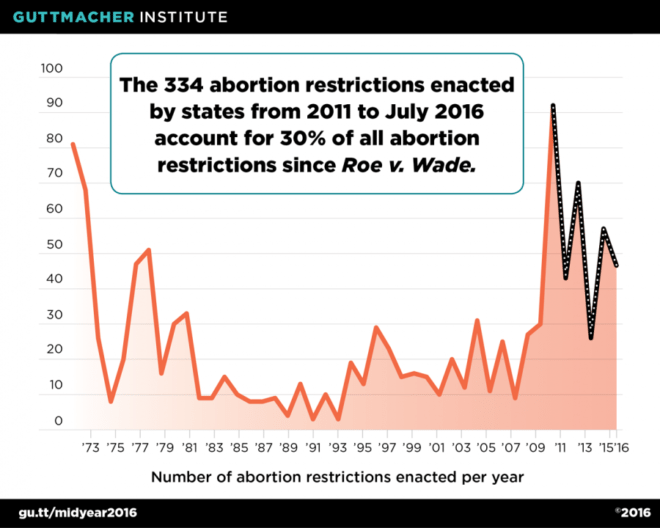
So far this year, legislators have introduced 1,256 provisions relating to sexual and reproductive health and rights. Of these, 35 percent (445 provisions) sought to restrict access to abortion services. By midyear, 17 states had passed 46 new abortion restrictions.
Including these new restrictions, states have adopted 334 abortion restrictions since 2010, constituting 30 percent of all abortion restrictions enacted by states since the U.S. Supreme Court decision in Roe v. Wade in 1973. However, states have also enacted 22 measures this year designed to expand access to reproductive health services or protect reproductive rights.
Signs of Progress
The first half of the year ended on a high note, with the U.S. Supreme Court handing down the most significant abortion decision in a generation. The Court’s ruling in Whole Woman’s Health v. Hellerstedt struck down abortion restrictions in Texas requiring abortion facilities in the state to convert to the equivalent of ambulatory surgical centers and mandating that abortion providers have admitting privileges at a local hospital; these two restrictions had greatly diminished access to services throughout the state (see Lessons from Texas: Widespread Consequences of Assaults on Abortion Access). Five other states (Michigan, Missouri, Pennsylvania, Tennessee, and Virginia) have similar facility requirements, and the Texas decision makes it less likely that these laws would be able to withstand judicial scrutiny (see Targeted Regulation of Abortion Providers). Nineteen other states have abortion facility requirements that are less onerous than the ones in Texas; the fate of these laws in the wake of the Court’s decision remains unclear.
Ten states in addition to Texas had adopted hospital admitting privileges requirements. The day after handing down the Texas decision, the Court declined to review lower court decisions that have kept such requirements in Mississippi and Wisconsin from going into effect, and Alabama Gov. Robert Bentley (R) announced that he would not enforce the state’s law. As a result of separate litigation, enforcement of admitting privileges requirements in Kansas, Louisiana, and Oklahoma is currently blocked. That leaves admitting privileges in effect in Missouri, North Dakota, Tennessee and Utah; as with facility requirements, the Texas decision will clearly make it harder for these laws to survive if challenged.
More broadly, the Court’s decision clarified the legal standard for evaluating abortion restrictions. In its 1992 decision in Planned Parenthood of Southeastern Pennsylvania v. Casey, the Court had said that abortion restrictions could not impose an undue burden on a woman seeking to terminate her pregnancy. In Whole Woman’s Health, the Court stressed the importance of using evidence to evaluate the extent to which an abortion restriction imposes a burden on women, and made clear that a restriction’s burdens cannot outweigh its benefits, an analysis that will give the Texas decision a reach well beyond the specific restrictions at issue in the case.
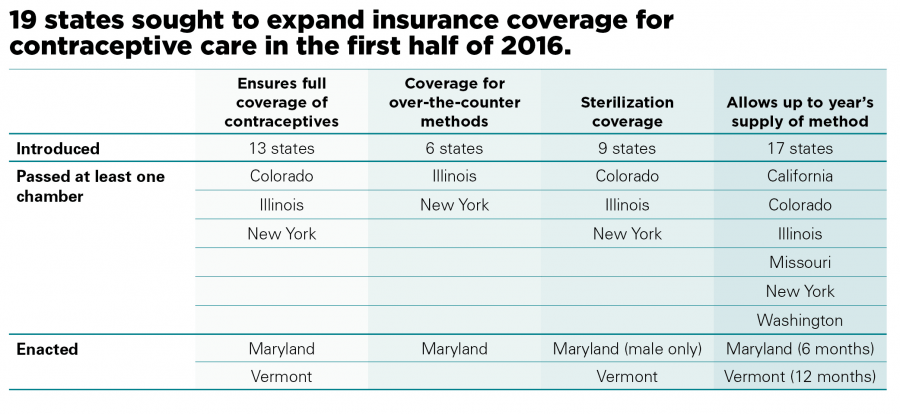
As important as the Whole Woman’s Health decision is and will be going forward, it is far from the only good news so far this year. Legislators in 19 states introduced a bevy of measures aimed at expanding insurance coverage for contraceptive services. In 13 of these states, the proposed measures seek to bolster the existing federal contraceptive coverage requirement by, for example, requiring coverage of all U.S. Food and Drug Administration approved methods and banning the use of techniques such as medical management and prior authorization, through which insurers may limit coverage. But some proposals go further and plow new ground by mandating coverage of sterilization (generally for both men and women), allowing a woman to obtain an extended supply of her contraceptive method (generally up to 12 months), and/or requiring that insurance cover over-the-counter contraceptive methods. By July 1, both Maryland and Vermont had enacted comprehensive measures, and similar legislation was pending before Illinois Gov. Bruce Rauner (R). And, in early July, Hawaii Gov. David Ige (D) signed a measure into law allowing women to obtain a year’s supply of their contraceptive method.
But the Assault Continues
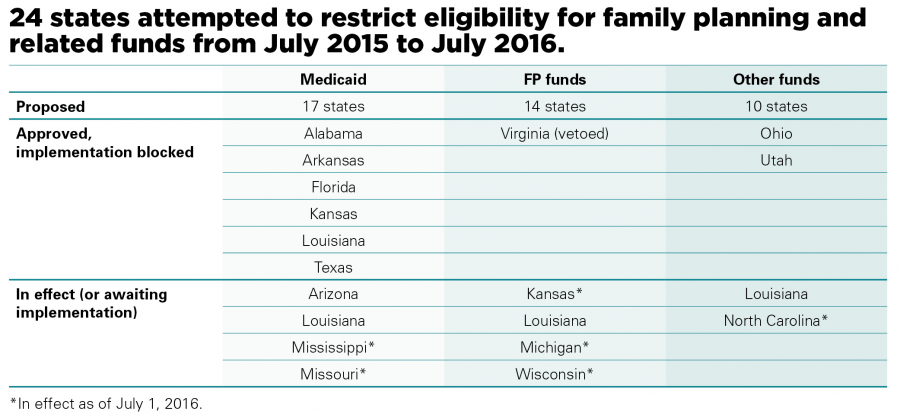
Even as these positive developments unfolded, the long-standing assault on sexual and reproductive health and rights continued apace. Much of this attention focused on the release a year ago of a string of deceptively edited videos designed to discredit Planned Parenthood. The campaign these videos spawned initially focused on defunding Planned Parenthood and has grown into an effort to defund family planning providers more broadly, especially those who have any connection to abortion services. Since last July, 24 states have moved to restrict eligibility for funding in several ways:
- Seventeen states have moved to limit family planning providers’ eligibility for reimbursement under Medicaid, the program that accounts for about three-fourths of all public dollars spent on family planning. In some cases, states have tried to exclude Planned Parenthood entirely from such funding. These attacks have come via both administrative and legislative means. For instance, the Florida legislature included a defunding provision in an omnibus abortion bill passed in March. As the controversy grew, the Centers for Medicare and Medicaid Services, the federal agency that administers Medicaid, sent a letter to state officials reiterating that federal law prohibits them from discriminating against family planning providers because they either offer abortion services or are affiliated with an abortion provider (see CMS Provides New Clarity For Family Planning Under Medicaid). Most of these state attempts have been blocked through legal challenges. However, a funding ban went into effect in Mississippi on July 1, and similar measures are awaiting implementation in three other states.
- Fourteen states have moved to restrict family planning funds controlled by the state, with laws enacted in four states. The law in Kansas limits funding to publicly run programs, while the law in Louisiana bars funding to providers who are associated with abortion services. A law enacted in Wisconsin directs the state to apply for federal Title X funding and specifies that if this funding is obtained, it may not be distributed to family planning providers affiliated with abortion services. (In 2015, New Hampshire moved to deny Title X funds to Planned Parenthood affiliates; the state reversed the decision in 2016.) Finally, the budget adopted in Michigan reenacts a provision that bars the allocation of family planning funds to organizations associated with abortion. Notably, however, Virginia Gov. Terry McAuliffe (D) vetoed a similar measure.
- Ten states have attempted to bar family planning providers’ eligibility for related funding, including monies for sexually transmitted infection testing and treatment, prevention of interpersonal violence, and prevention of breast and cervical cancer. In three of these states, the bans are the result of legislative action; in Utah, the ban resulted from action by the governor. Such a ban is in effect in North Carolina; the Louisiana measure is set to go into effect in August. Implementation of bans in Ohio and Utah has been blocked as a result of legal action.
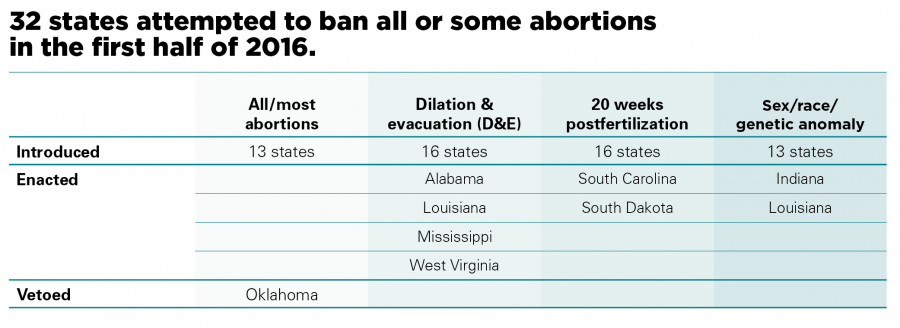
The first half of 2016 was also noteworthy for a raft of attempts to ban some or all abortions. These measures fell into four distinct categories:
- By the end of June, four states enacted legislation to ban the most common method used to perform abortions during the second trimester. The Mississippi and West Virginia laws are in effect; the other two have been challenged in court. (Similar provisions enacted last year in Kansas and Oklahoma are also blocked pending legal action.)
- South Carolina and North Dakota both enacted measures banning abortion at or beyond 20 weeks post-fertilization, which is equivalent to 22 weeks after the woman’s last menstrual period. This brings to 16 the number of states with these laws in effect (see State Policies on Later Abortions).
- Indiana and Louisiana adopted provisions banning abortions under specific circumstances. The Louisiana law banned abortions at or after 20 weeks post-fertilization in cases of diagnosed genetic anomaly; the law is slated to go into effect on August 1. Indiana adopted a groundbreaking measure to ban abortion for purposes of race or sex selection, in cases of a genetic anomaly, or because of the fetus’ “color, national origin, or ancestry”; enforcement of the measure is blocked pending the outcome of a legal challenge.
- Oklahoma Gov. Mary Fallin (R) vetoed a sweeping measure that would have banned all abortions except those necessary to protect the woman’s life.
In addition, 14 states (Alaska, Arizona, Florida, Georgia, Idaho, Indiana, Iowa, Kentucky, Louisiana, Maryland, South Carolina, South Dakota, Tennessee and Utah) enacted other types of abortion restrictions during the first half of the year, including measures to impose or extend waiting periods, restrict access to medication abortion, and establish regulations on abortion clinics.
Zohra Ansari-Thomas, Olivia Cappello, and Lizamarie Mohammed all contributed to this analysis.