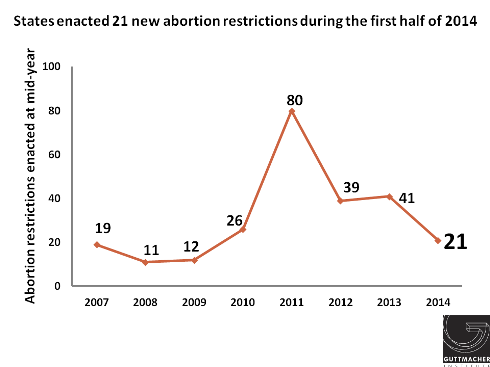
So far this year, 13 states have adopted 21 new restrictions that could limit access to abortion. These restrictions range from requirements that abortion providers have admitting privileges at local hospitals to bans on insurance coverage to limitations on medication abortion. At the same time, and building on momentum from last year, three states moved to protect access to abortion services, while four states and the District of Columbia took steps to improve access to other reproductive health services.
So far this year, 21 new abortion restrictions have been enacted, about half the number (41) that had been enacted by this point last year. Several reasons exist for this drop. Some of the decline is the result of regular cyclical trends, as states historically have shorter sessions in election years and some state legislatures that have been particularly active on abortion issues (Montana, Nevada, North Dakota and Texas) are not in session in even-number years (see A Surge of State Abortion Restrictions Puts Providers—and the Women They Serve—in the Crosshairs). In addition, an array of other issues (responses to the heroin epidemic, the expansion of full-benefit Medicaid as allowed by the Affordable Care Act (ACA), the common core educational initiative and minimum wage increases) moved to the front burner in many legislatures, perhaps limiting legislative attention to abortion.
Nonetheless, access to abortion will become even more difficult in many states because of actions taken this year and, once again, restrictions known as targeted regulations of abortion providers (TRAP), are taking center stage (see TRAP Laws Gain Political Traction While Abortion Clinics—and the Women They Serve—Pay the Price).
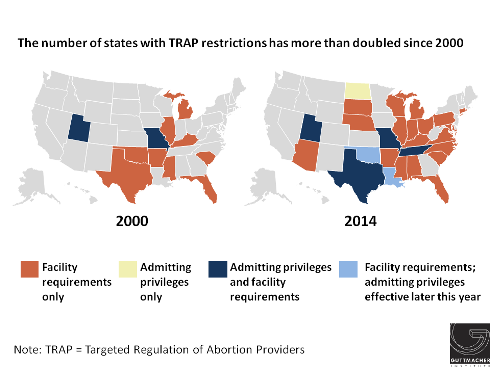
Perhaps spurred by a decision handed down by the U.S. Court of Appeals for the Fifth Circuit upholding a Texas law, Louisiana and Oklahoma enacted measures requiring abortion providers to have admitting privileges at a local hospital. Once these two new laws go into effect later in the year, seven states will require abortion providers to have admitting privileges (see Targeted Regulation of Abortion Providers). In addition, Arizona and Indiana, which already had stringent requirements on facilities where abortions are performed, moved to allow the state health agency to make unannounced inspections. Altogether, 26 states have some sort of TRAP law, a sharp increase from 2000, when only 11 states had such requirements. With the addition of these new laws, 59% of women of reproductive age live in a state that has enacted TRAP provisions.
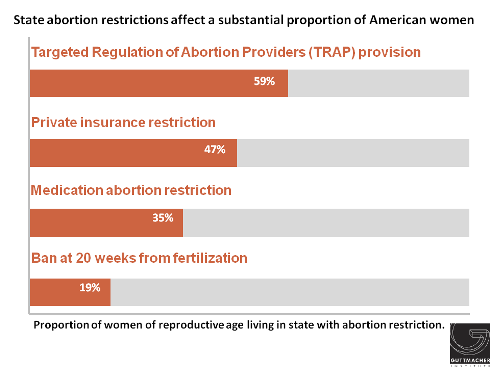
In contrast to the momentum gained as a result of court actions on TRAP requirements, interest in banning abortion at about 20 weeks postfertilization may have been dampened by court rulings. In January, the U.S. Supreme Court declined to review a lower court decision striking down an Arizona law banning abortion at 18 weeks postfertilization based on the notion that a fetus feels pain at that point in pregnancy. In 2013, three such bans were enacted (and 11 have been enacted since 2010). This year, however, only Mississippi enacted this type of measure. West Virginia Gov. Earl Ray Tomblin (D) vetoed a similar measure. Including Mississippi, 10 states have laws in effect that ban abortion at about 20 weeks postfertilization (see State Policies on Later Abortion).
Similarly, the Supreme Court refused to review a state court ruling striking down a ban on medication abortion in Oklahoma. (That action did not affect a separate state ban on the use of telemedicine to provide the medication.) Following the Court’s ruling, the state enacted a measure mandating use of the outdated FDA-approved protocol that requires higher doses of the medication, has an increased risk of side effects and is more expensive; this new restriction goes into effect in November (see Medication Abortion Restrictions Burden Women and Providers—and Threaten U.S. Trend Toward Very Early Abortion). So far this year, Oklahoma is the only state to restrict access to medication abortion, compared with seven that did so in 2013. Currently, 16 states limit access to medication abortion (see Medication Abortion) including 15 that bar use of telemedicine and two that require use of the outdated FDA protocol (Texas is the only state that has both types of restrictions in effect).
Two states have adopted restrictions on insurance coverage of abortion so far this year. Georgia moved to limit coverage in policies sold on the insurance exchange established under the Affordable Care Act to cases of life endangerment and significant risk to the woman’s health, and codify what had been a similar administrative policy that prohibits abortion coverage in the health plan for state employees except when the woman’s life is endangered. Similarly, Indiana, which had already restricted coverage on the exchange to instances of life endangerment, rape, incest and significant risk to the woman’s health, expanded its restriction to apply to any private insurance policy purchased in the state. A total of 25 states restrict coverage of abortion in private insurance plans (see Restricting Insurance Coverage of Abortion).
South Dakota enacted a new provision to ban abortion for purposes of sex selection. This new law brings to seven the number of states with such a ban (see A Problem-and-Solution Mismatch: Son Preference and Sex-Selective Abortion Bans).
Eight states moved to expand existing abortion restrictions:
- Three states enacted measures to expand longstanding abortion counseling requirements. Kansas removed a requirement that counseling materials be medically accurate. A new law in Louisiana requires counseling materials to include information on the “psychological harms” of abortion. And a law passed in Oklahoma requires women seeking an abortion in cases of a diagnosed fetal abnormality to be given information on the availability of perinatal hospice care; it also requires abortion providers to report to the state that the counseling was provided. Twenty-seven states have abortion counseling requirements (see Counseling and Waiting Periods for Abortion).
- Alabama extended the waiting period for women seeking an abortion from 24 to 48 hours. The state joins South Dakota and Utah in having a waiting period longer than 24 hours; those two other states require a woman to wait 72 hours. Twenty-six states require a waiting period for a woman seeking an abortion (see Counseling and Waiting Periods for Abortion). (Missouri Gov. Jay Nixon (D) vetoed a 72-hour waiting period bill in early July.)
- A new law in Arizona criminalizes helping a minor to obtain an abortion without parental consent. Alabama added three new provisions to its existing parental consent statute. First, the law requires a parent seeking to consent to an abortion for his or her daughter to provide a certified birth certificate, along with other documents, as proof that he or she is the minor’s parent. Second, the law requires a minor seeking a judicial waiver of the parental consent requirement to provide “reliable evidence” as to the need for the abortion and demonstrate that she is sufficiently mature to decide for herself whether to have an abortion. Finally, the law requires that the office of the state attorney general participate in any hearing to determine whether a judicial bypass will be granted. Thirty-eight states require parental involvement for a minor seeking an abortion (see Parental Involvement in Minors’ Abortions).
- Alaska limited the situations in which Medicaid funding is available for abortion services for low-income women. The state has long been required by state court to cover abortions when medically necessary. The new law, which is being challenged in court, includes a specific definition for “medical necessity” that reduces the circumstances in which funding is available. (In addition, Maryland re-enacted its longstanding restriction on public funding for abortion services as part of its annual budget bill.) Seventeen states fund all or most medically necessary abortions (see State Funding of Abortion Under Medicaid).
- Florida amended its restrictions on later abortion to permit the procedure after viability only when the woman’s life or physical health is threatened; previously, the health exception was not limited to “physical” health, so that it also allowed a woman to obtain an abortion if her mental health was in jeopardy (see State Policies on Later Abortions).
- In a move aimed at restricting information about abortion, a new law in Virginia allows genetic counselors to refuse to provide any information to patients because of their personal religious or moral beliefs.
At the same time, however, three states have moved to expand or protect access to abortion services so far this year:
- In early June, New Hampshire adopted a law that would establish a buffer zone of up to 25 feet around clinic entrances. (The law came before the Supreme Court decision in McCullen v. Coakley in late June that invalidated a 35-foot buffer zone in Massachusetts; the impact of this ruling on the New Hampshire law is still to be determined.) Two other states, Colorado and Montana, have so-called floating buffer zones that prohibit a protester from getting within eight feet of a patient when the patient is within a specified distance from the clinic (see Protecting Access to Clinics); these floating zones were upheld by the Court in 2000.)
- In March, Utah moved to remove obstacles to obtaining an abortion in cases of fetal impairment by waiving counseling requirements in those cases.
- In April, Vermont repealed its pre-Roe abortion ban; the move would protect access to abortion services in the event Roe is overturned (see Abortion Policy in the Absence of Roe).
Four states and the District of Columbia took steps to expand access to other sexual and reproductive health services. A new law in Maryland seeks to provide access to confidential care for individuals insured as dependents on someone else’s insurance policy, such as a parent or spouse; the law is similar to one enacted in California in 2013 (see A New Frontier in the Era of Health Reform: Protecting Confidentiality for Individuals Insured as Dependents). The District of Columbia joined 28 states to allow health care practitioners to provide at least some STI treatment for the partner of a patient diagnosed with an STI without first examining the partner (see Partner Treatment for STIs). Finally, three states—Connecticut, New Mexico and South Carolina—expanded requirements for sex education; a new law in Connecticut requires education on dating violence and the laws in New Mexico and South Carolina require education on sexual abuse (see Sex and HIV Education).