In most years, state legislative action on reproductive health and rights issues winds down as states approve their budgets for the fiscal year beginning July 1. In contrast, this year a handful of states, including Texas and Wisconsin, are likely to continue debating these issues for weeks, and perhaps months, after adopting their budgets. Altogether, legislatures in 11 states and the District of Columbia remain in session.
In the first six months of 2013, states enacted 106 provisions related to reproductive health and rights; issues related to abortion, family planning funding and sex education were significant flashpoints in several legislatures. Although initial momentum behind banning abortion early in pregnancy appears to have waned, states nonetheless adopted myriad restrictions on access to abortion. However, this year is notable also for positive action on other reproductive health issues in a few states, including important new provisions enacted to expand access to comprehensive sex education, expedited partner treatment for STIs and emergency contraception for women who have been sexually assaulted.
Browse the status of state laws on key reproductive health and rights issues.
Explore state legislative activity around sexual and reproductive health issues.
For a table showing legislation enacted in 2013, click here.
Abortion Restrictions
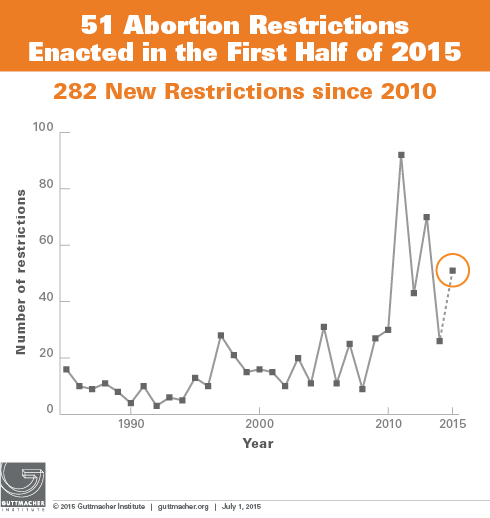
So far this year, legislators have enacted 43 provisions aimed at restricting access to abortion. Although this is significantly lower than the record-breaking 80 restrictions that had been enacted by this point in 2011, it is nonetheless a higher number of restrictions than in any year other than 2011 and as many as enacted in all of 2012.
Early in the 2013 legislative year, it appeared that antiabortion activity would focus on banning abortion early in pregnancy, either by declaring that personhood begins at the moment of conception or by banning the procedure outright. Indeed, provisions banning early abortion were enacted in two states in March alone. First, the Arkansas legislature overrode a veto by Gov. Mike Beebe (D) to ban abortions occurring more than 12 weeks after a woman’s last menstrual period; in May, a federal judge temporarily blocked enforcement of the law. Later in March, North Dakota enacted a ban on abortions occurring after a fetal heartbeat is detected, which generally occurs at about six weeks after a woman’s last menstrual period; although a legal challenge has been filed, the law is scheduled to go into effect in August. The North Dakota legislature also approved an initiative that will be placed on the November 2014 ballot to define a person as a “human being at any stage of development;” if approved by voters, it could restrict women’s access to birth control and abortion services. Although legislation to ban early abortion had been introduced in 13 other states (AL, CO, FL, IA, KS, KY, MO, MS, OK, SC, VA, WA, WY) during the first half of the year, none was passed by a legislative chamber.
Although the momentum for banning early abortion appears to have slowed, the same cannot be said for bans on abortion later in pregnancy. Legislation to ban nearly all abortions performed at or beyond 20 weeks postfertilization (the equivalent of 22 weeks after the woman’s last menstrual period) has been enacted in Arkansas and North Dakota this year. (Notably, these two states also moved to bar abortion early in pregnancy.) These provisions are based on the spurious belief that the fetus can feel pain at that point of development. Including Arkansas and North Dakota, bans on abortion at or after 20 weeks have been enacted in 10 states, while an eleventh, Arizona, bans abortion at 18 weeks postfertilization; enforcement of three of these provisions has been enjoined pending legal challenges (see State Policies on Later Abortions). In addition, the Texas legislature is continuing a high-profile debate on a similar proposal, and a measure that would ban abortion at or after 20 weeks nationwide was adopted by the U.S. House of Representatives in June, although it has no chance of becoming law.
Moreover, several states returned to familiar territory and approved a plethora of restrictions that, while stopping short of banning abortion, would nonetheless significantly hamper women’s access to the procedure.
- Five states moved to impose targeted regulation of abortion providers (TRAP) in the first half of 2013. These laws are designed to discourage medical professionals from providing abortion and make it impossible for clinics to remain open (see TRAP Laws Gain Political Traction While Abortion Clinics—and the Women They Serve—Pay the Price). Alabama and North Dakota enacted laws that require providers to have admitting privileges at a local hospital, effectively giving hospitals veto power over clinics’ ability to provide services. This brings to seven the number of states requiring abortion providers to have hospital privileges, although two of these laws are not yet in effect and enforcement of two is blocked pending the outcome of a legal challenge (see Targeted Regulation of Abortion Providers).
Ohio has long required abortion providers to have an agreement with a hospital allowing them to transfer patients needing emergency care. In June, Ohio adopted a new provision prohibiting public hospitals in the state from entering into these transfer agreements, which will make it difficult for some clinics to remain in operation. Including Ohio, nine states require abortion providers to have transfer agreements, requirements that do little to add to existing patient safeguards ensuring hospital care in the event of an emergency.
In addition, Alabama approved new standards for abortion clinics that are essentially the same as those required for ambulatory surgical centers (ASCs), even though the latter provide procedures that are more invasive and risky than abortion. Indiana, which had already required sites where surgical abortion was performed to adhere to standards similar to those for ASCs, extended these requirements to apply to sites where only medication abortion is performed. Virginia, meanwhile, finalized regulations to implement its 2011 TRAP law that requires clinics to meet stringent standards equivalent to those for ASCs. Including these new requirements, 26 states require abortion facilities to meet the same standards as those required for ASCs. - Four states limited provision of medication abortion by prohibiting the use of telemedicine, which is rapidly becoming a widely used tool for expanding access to health care, particularly in rural areas (see Medication Abortion Restrictions Burden Women and Providers—and Threaten U.S. Trend Toward Very Early Abortion). Alabama, Indiana, Louisiana and Mississippi enacted laws that require the physician prescribing the medication to be in the same room as the patient, bringing to 12 the number of states that prohibit the use of telemedicine for this procedure, although enforcement of the provision in Wisconsin has been enjoined by a state court (see Medication Abortion).
- Arkansas and Pennsylvania moved to limit coverage of abortion in the health exchanges that will be established under the Affordable Care Act. Including these new provisions, 22 states have moved to restrict abortion coverage available through state insurance exchanges (see Restricting Insurance Coverage of Abortion).
- States also adopted several other provisions designed to reduce access to abortion. These include measures that require a woman seeking an abortion to have an ultrasound (Indiana); require a woman to undergo testing to determine whether a fetal heartbeat is audible (Ohio); extend the amount of time a woman must wait to have an abortion by excluding weekends and holidays from the days counted toward South Dakota’s 72-hour waiting period; and allow health care providers to withhold information about a woman’s pregnancy if they are concerned that it might lead her to consider abortion (Kansas and Montana).
Family Planning Funding
Although the majority of state legislation hostile to reproductive rights focused on abortion in 2013, two states acted to limit access to family planning services. Ohio and Oklahoma moved to bar providers that specialize in the provision of family planning services and that are not affiliated with health departments from being able to receive funding that flows through the states’ treasuries. Oklahoma’s budget excludes family planning providers from being able to receive state family planning funds along with Title X dollars or federal maternal and child health or social services block grant funds. Ohio established a priority system for allocating state or federal funds (including Title X dollars) that puts family planning providers at the end of a long list that includes health departments and community health centers. These moves continue a disturbing trend that began in 2011.
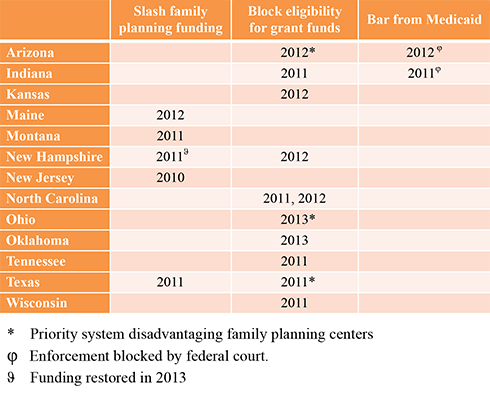
At the same time, states and courts took steps to protect access to family planning services in three states during the first half of 2013. New Hampshire’s budget reversed the 57% cut to family planning funding adopted in 2011, restoring funds to their previous level. Federal courts, meanwhile, sided with the Obama administration and blocked provisions adopted in Arizona and Indiana that would have excluded family planning providers that had any association with abortion from being able to participate in the massive Medicaid program (see Besieged Family Planning Network Plays Pivotal Role).
Positive Movement on Prevention
Five states took positive steps during the first half of the year by enacting measures that expand access to comprehensive sex education and reproductive health care.
- Colorado and Illinois enacted laws aimed at improving sex education for adolescents. Colorado adopted a measure to require all sex education provided in the state to be scientifically proven to delay sexual debut, reduce adolescents’ number of sexual partners and sexual frequency, or increase their contraceptive use. A law enacted in Illinois requires students to receive instruction on sexual abuse (see Sex and HIV Education).
- Nebraska enacted a law that allows medical providers to prescribe or dispense a drug for treatment of certain STIs for a patient’s partner without first seeing the partner. Vermont, which already permitted partner treatment for Chlamydia, amended its law to apply to a broader range of STIs. Nebraska is the 27th state to permit expedited partner therapy (see Partner Treatment for STIs).
- Hawaii enacted a measure requiring hospitals treating women who have been sexually assaulted to provide them with medically accurate and unbiased information on emergency contraception, and to give them the medication upon request. Hawaii is the 17th state, along with the District of Columbia, to require that a woman be given information about emergency contraception and the 13th state (including the District of Columbia) to require that she be given the medication on request (see Emergency Contraception).