Telehealth has become an increasingly critical lifeline for health equity, including in the realm of reproductive health care, and specifically in abortion care. Telehealth enables clinicians to treat patients virtually without an in-person appointment. Patients can connect directly with a health care provider from any location using video or phone calls (often referred to as synchronous care), or via secure chat or messaging (asynchronous care). Telehealth can provide essential medical services directly to patients in their homes, between clinical sites, or through a hybrid of in-person and virtual care. These different modalities of telehealth can also serve important functions for abortion care.
A substantial body of research shows that telehealth can be used to safely and effectively deliver some services without the need for in-person clinical visits. In particular, research has shown that telehealth for medication abortion is just as safe and effective as in-person care. Telehealth can help make comprehensive reproductive health care more readily available, accessible and patient-centered, regardless of a person’s location or their local clinical infrastructure.
Since the COVID-19 pandemic, the use of telehealth has accelerated rapidly. As of 2022, roughly 39% of US adults reported using telehealth in the past year, with similar use rates across age, race, ethnicity and income. In 2024, some 71% of physicians reported using telehealth in their practice weekly—up from about 25% in 2018. This increase in the general prevalence of telehealth has been mirrored in the provision of abortion care, with the latest data showing that 29% of abortions are now provided via telehealth.
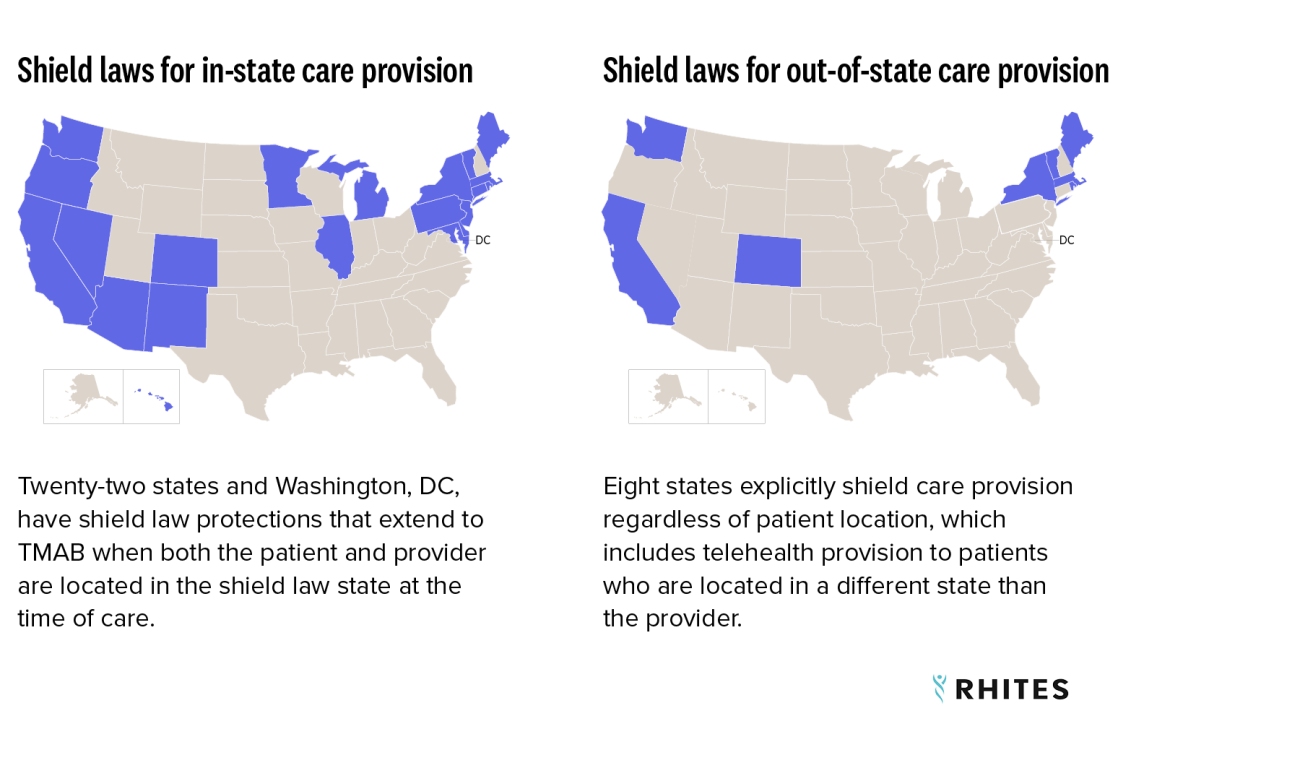
The expansion of telehealth abortion care has been shaped by shifts in federal and state policy. Since 2023, after an exhaustive review of the research on safety and efficacy, the Food and Drug Administration (FDA) has allowed telehealth, mail and pharmacy provision of mifepristone, one of two drugs used in the most common medication abortion regimen. In addition, eight states have passed shield laws that explicitly protect clinicians who provide telehealth abortion care to patients in states with total bans and other severe restrictions. However, anti-abortion activists have responded aggressively to the growing prevalence of telehealth for medication abortion and have challenged these evidence-based policies through legislation and in the federal courts. As a result, understanding the various models of telehealth abortion care is more important than ever.
What Is Telehealth for Medication Abortion?
Medication abortion is a method of ending a pregnancy using pharmaceutical drugs. In the United States, this most commonly involves a two-drug regimen: mifepristone (an antiprogestin that blocks the hormone needed to sustain the pregnancy) followed by misoprostol (a prostaglandin that causes the uterus to contract and expel the pregnancy). Other drug regimens (such as misoprostol alone) can also be a safe and effective way to end a pregnancy.
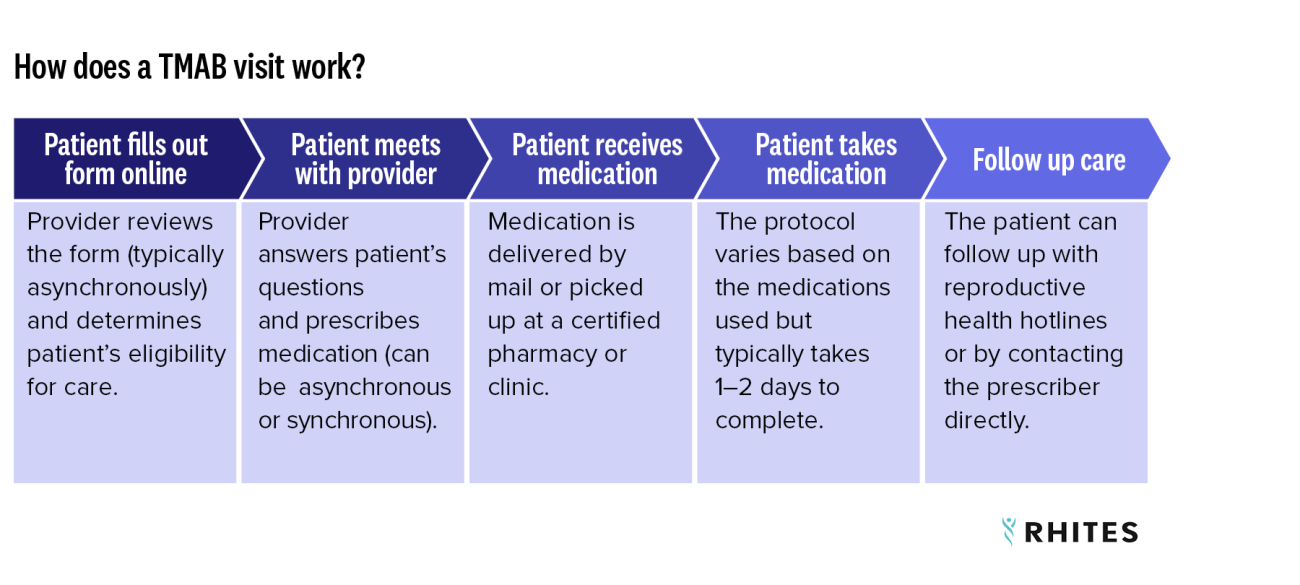
Telehealth for Medication Abortion (TMAB) generally refers to the use of phone and/or video calls for some or all of the interactions needed to prescribe and receive medication abortion pills. TMAB can be direct-to-patient, site-to-site, or accessed through a hybrid in-person/virtual care experience using different modalities.
How Can Telehealth Be Used to Provide Medication Abortion?
Direct to patient:
- The provider and patient are located in different places while using either a secure video-conferencing platform, audio platform, or an (asynchronous) messaging system. This is a fully remote model and often the patient is located outside of a clinical setting, such as in their home.