
2016 Brought a Flood of Abortion Restrictions, But Also a Surge of Proactive Measures
While state legislators pushed through 20-week abortion bans and restrictions against fetal-tissue research in some states, there was progress on measures related to contraceptive access in places such as California, Illinois, and Vermont.

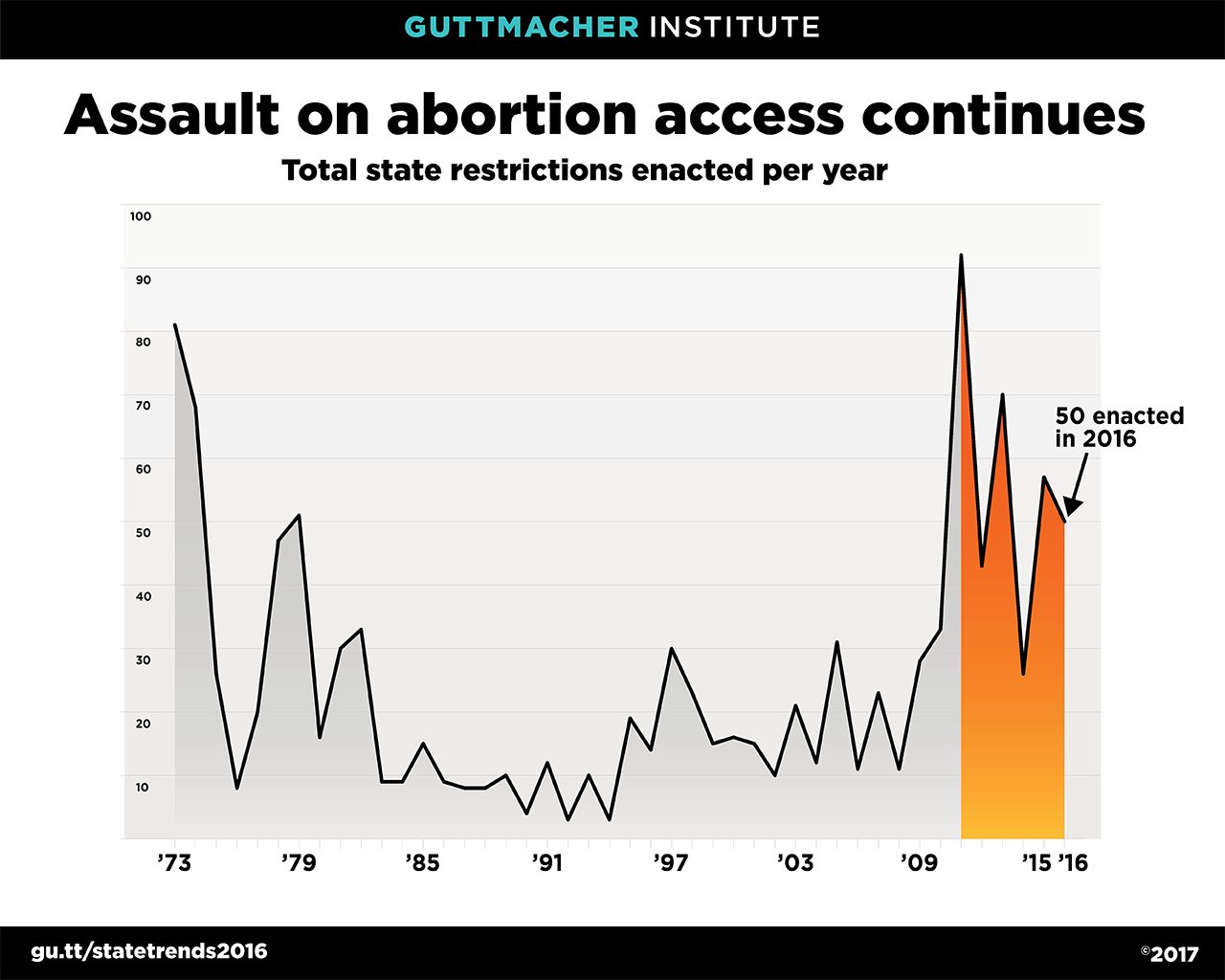
In 2016, 18 states enacted 50 new abortion restrictions, bringing the number of new abortion restrictions enacted since 2010 to 338. Although state-level assaults on abortion access continued, 16 states took important steps in 2016 to expand access to other sexual and reproductive health services, adopting a total of 28 proactive measures. Many of these measures expand access to contraception by requiring health plans to cover an extended supply of contraceptive methods (five states), authorizing pharmacists to dispense contraceptives without a physician’s prescription (one state), or expanding insurance coverage of contraception (three states).
Aside from legislation, the most notable event of 2016 related to reproductive health access was the U.S. Supreme Court’s decision in Whole Woman’s Health v. Hellerstedt in June. That decision struck down Texas restrictions that had required abortion facilities to be the equivalent of ambulatory surgical centers and mandated abortion providers have admitting privileges at a local hospital; these measures had greatly diminished access to services in the state. Notably, the Court’s ruling underscored the need to consider scientific evidence, and not just lawmakers’ beliefs, in evaluating the constitutionality of abortion restrictions.
Unfortunately, just months after that landmark ruling, the election of Donald J. Trump raised the specter that the Supreme Court—if dramatically reconfigured by the new administration—could place abortion rights very much in jeopardy across the country. Moreover, the resurgent Republican Party—having maintained anti-abortion majorities in both chambers of Congress—is undoubtedly planning an aggressive assault on sexual and reproductive health and rights. The Republican platform adopted in 2016 takes its cue from the states, naming many of the abortion restrictions that have received the most attention from state legislators in 2016, including banning abortions at 20 weeks post-fertilization, outlawing dilation and evacuation abortion, restricting fetal tissue donation and research, and banning abortion for purposes of sex selection and genetic anomaly.
Trump’s victory also threatens the federal contraceptive coverage guarantee included in the Affordable Care Act (ACA). Overturning the ACA overall is a key goal of the incoming administration; more specifically, Vice President-elect Mike Pence has repeatedly promised action on the contraceptive coverage guarantee. Regardless of how this drama plays out in the coming months, states will continue to have a critical role to play. Twenty-eight states have a state-level contraceptive coverage guarantee. Most of these measures require insurers to cover the full range of FDA-approved methods, and laws in California, Illinois, Maryland, and Vermont require this coverage with no cost sharing. Expanding insurance coverage of contraceptive services under private insurance has been a significant focus of state legislators supportive of women’s reproductive health care; in the last three years, those same four states have moved to expand access to contraceptive coverage in some form.
Restricting Abortion Access
The 338 state abortion restrictions adopted since 2010—the year anti-abortion forces took control of many state legislatures and governors’ mansions—account for 30 percent of the 1,142 abortion restrictions enacted by states since the 1973 Supreme Court decision in Roe v. Wade. These restrictions greatly shape the landscape facing women seeking to access abortion care.
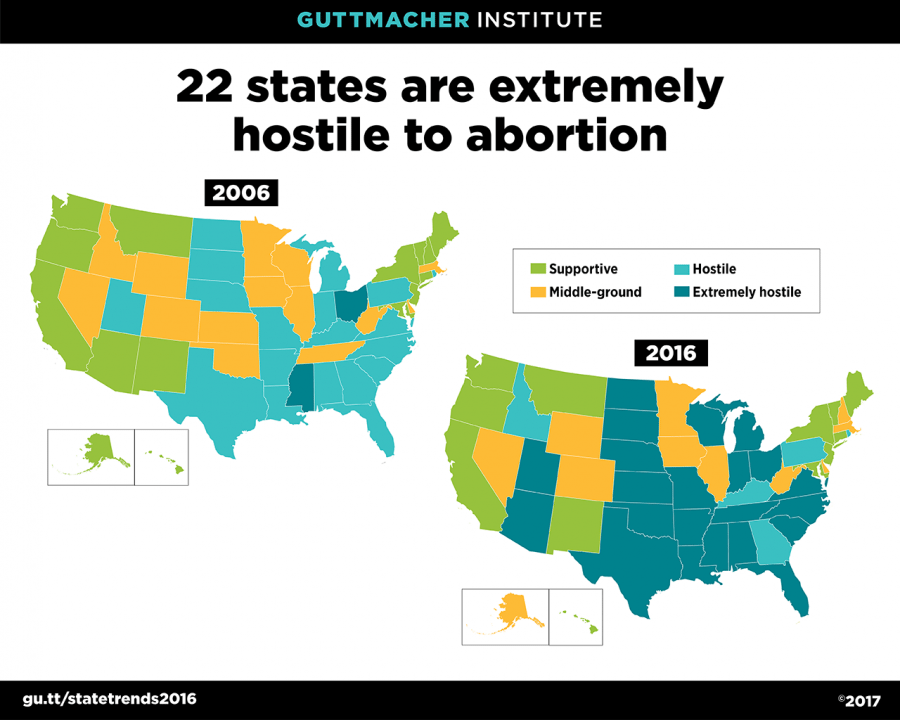
By 2016, more than half of all states had at least four of the ten major types of abortion restrictions and so are considered hostile to abortion rights. Notably, nearly all the states in the South, along with most of those in the Midwest, are considered hostile. Twenty-two states have six or more restrictions, enough to be classified as extremely hostile to abortion rights.
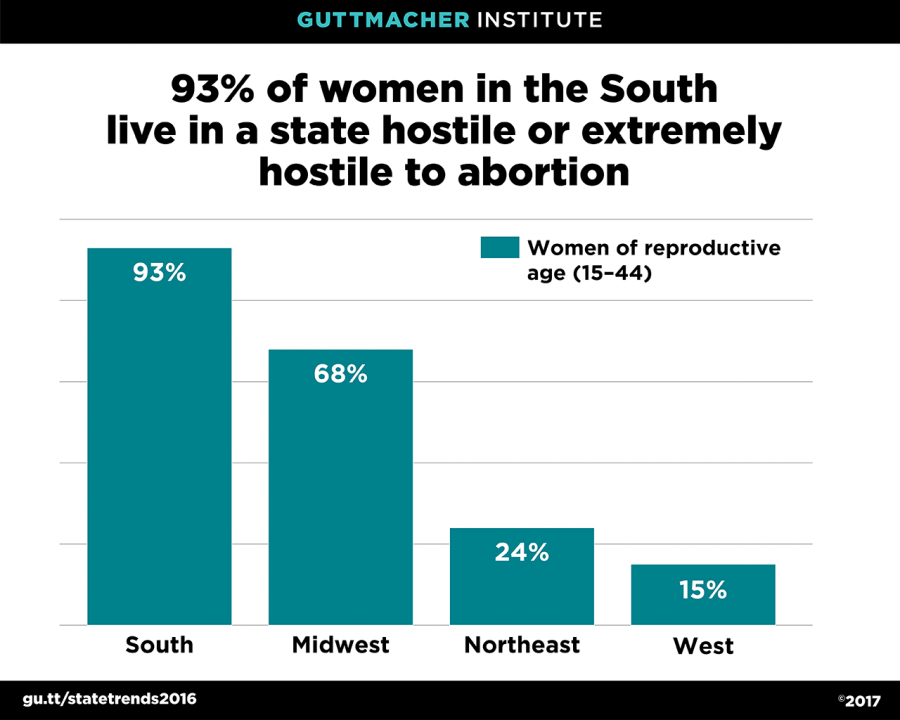
In 2016, 57 percent of American women of reproductive age (15 to 44) lived in a state considered either hostile or extremely hostile to abortion rights. Only 30 percent of women lived in a state supportive of abortion rights (a state with no more than one type of restriction), and 13 percent lived in a middle-ground state (a state with two or three restrictions). For the 38 percent of all reproductive-age women who live in the South, chances of living in a state supportive of abortion rights are particularly low: Only 5 percent live in a supportive state (Maryland), while 93 percent live in a state that is hostile or extremely hostile to abortion rights. By contrast, 62 percent of women in the Northeast live in a supportive state, and only 24 percent of women in that region live in a state that is considered hostile.
Five abortion-related topics received particular attention from state lawmakers in 2016:
- Banning dilation and evacuation abortion. Four states (Alabama, Louisiana, Mississippi, and West Virginia) banned the use of dilation and evacuation, a common and medically proven method of second-trimester abortion. The new laws in Alabama and Louisiana, along with laws that were passed in 2015 in Kansas and Oklahoma, are not in effect pending the outcome of litigation. Bans are in effect in Mississippi and West Virginia.
- Restricting fetal tissue donation and research. In the aftermath of the discredited videos targeting Planned Parenthood clinics, eight states (Arizona, Florida, Idaho, Indiana, Louisiana, Michigan, South Dakota, and Tennessee) enacted measures limiting fetal tissue donation; seven of them (all except Michigan) also banned research involving tissue from an abortion. The provisions in Louisiana are not in effect pending the outcome of litigation.
- Banning abortion for specific circumstances. Indiana and Louisiana enacted laws that would have banned abortion due to a genetic anomaly. Neither law is in effect due to ongoing litigation, leaving North Dakota as the only state with such a ban in effect. The Indiana law would also have banned abortion based on the race or sex of the fetus or because of the fetus’s color, national origin, or ancestry. Seven states (Arizona, Kansas, North Carolina, North Dakota, Oklahoma, Pennsylvania, and South Dakota) have laws in effect banning abortion due to the sex of the fetus; Arizona’s law also bans abortion for purposes of race selection.
- Banning abortion at 20 weeks post-fertilization. Ohio, South Carolina, and South Dakota enacted measures that ban abortion at 20 weeks post-fertilization (equivalent to 22 weeks after the woman’s last menstrual period). All of these new laws permit an abortion after that point when the woman’s life is endangered or if she has a severe physical health complication; the South Carolina law also permits an abortion in the case of a lethal fetal anomaly. Fifteen states, including South Carolina and South Dakota, have similar restrictions in effect. The Ohio restriction is scheduled to take effect later this year.
- Requiring fetal tissue to be cremated or buried. Indiana and Louisiana enacted provisions that would have required tissue from an abortion to be cremated or buried; Texas adopted similar requirements through administrative regulations. None of the requirements are in effect due to legal action.
Making Proactive Progress
Between 2001 and 2016, states have enacted 214 legislative measures aimed at expanding access to abortion, contraception, and related services and education. Two-thirds of these provisions fall into five categories: comprehensive sex education (44 measures), contraceptive coverage (30 measures), access to emergency contraception (25 measures), Medicaid family planning expansions (20 measures), and expedited partner treatment for STIs (18 measures). The remaining proactive measures address issues such as criminalizing violence at abortion clinics; repealing pre-Roe abortion restrictions; expanding access to family planning services; requiring insurance coverage of infertility and STI services; protecting enrollee confidentiality with regard to medical care; and allowing minors to consent to reproductive health-care services.

Efforts to make proactive progress picked up dramatically in 2013, after a considerable lull in 2010-2012. Significantly, the 28 proactive measures enacted in 2016 represent the highest number of proactive measures on reproductive health issues enacted in state legislatures in the past 16 years.
Expanding access to contraception was a particular focus of legislators in 2016, with three types of measures commanding major attention:
Extended contraceptive supply. Five states enacted new laws in 2016 that allow a woman to obtain an extended supply of her contraceptive method from a pharmacy; health plans typically limit access to a one-month or three-month supply. The new provisions in California, Hawaii, Illinois, and Vermont allow women to receive up to a year’s worth of their method. The Maryland law allows women to obtain up to a six-month supply. With the addition of these states, a total of six states and the District of Columbia will now require health plans to cover an extended supply.
Access to contraceptives without a prior prescription. In 2014, California enacted a measure authorizing pharmacists to dispense contraceptives without a prescription from a clinician. In 2016, the state expanded this provision to permit Medicaid coverage of methods dispensed by pharmacists without a prior prescription. Oregon, Washington state, and the District of Columbia already have similar laws in place.
Contraceptive coverage. Three states amended their state laws requiring contraceptive coverage to more closely mirror, and build on, the federal contraceptive coverage guarantee included in the Affordable Care Act. Illinois, Maryland, and Vermont adopted new laws that require coverage of all FDA-approved methods, ban the use of techniques such as prior authorization that insurers use to limit coverage, and prohibit cost sharing for contraceptives. Including these states, 28 states have similar laws mandating contraceptive coverage in health plans.
Zohra Ansari-Thomas, Olivia Cappello, and Lizamarie Mohammed all contributed to this analysis.