
On his first business day in office—and two days after unprecedented national and global protests by women’s rights supporters—President Trump signed an executive policy to expand antiabortion restrictions in U.S. foreign aid. The global gag rule, also known originally as the Mexico City policy, was first implemented in 1984 to halt U.S. assistance for family planning programs overseas to foreign nongovernmental organizations (NGOs) that used non-U.S. government funding to provide abortion services, information, counseling or referrals or to advocate for liberalizing or otherwise improving their country’s abortion laws (see "The Global Gag Rule and Fights Over Funding UNFPA: The Issues That Won’t Go Away," Spring 2015). Proponents of the gag rule claimed that such a policy kept U.S. funding from supporting abortion, knowing full well that no U.S. foreign assistance funds have been spent on abortion since the Helms Amendment was enacted in 1973.
The Trump-Pence administration escalated the impact of the gag rule by expanding its application from international family planning funding to all "global health assistance furnished by all departments or agencies."1 After weeks of confusion and alarm, the administration released guidance in March to implement the policy, but only for recipients of international family planning assistance.2 These guidelines essentially mirrored the 2001 provisions issued by the Bush administration. On May 15, the Trump administration finally announced the expanded guidance, which renamed the policy as Protecting Life in Global Health Assistance and clarified that the policy now applies at the very least to global health assistance appropriated under the State Department, the U.S. Agency for International Development (USAID) and the Department of Defense.3
The global gag rule threatens the provision of health services in developing countries. Whether intended or not, the architects of the Trump global gag rule have created a policy that will disrupt and reverse the United States’ long-held development goal of improving health worldwide. The vast global health portfolio, supported by billions of dollars of U.S. funding, covers health-related activities in about 60 low- and middle-income countries, including programs on HIV/AIDS, Zika, maternal and child health, malaria, nutrition and others.4 International development and health experts have sounded the alarm that these programs will suffer in the future as have reproductive health programs in the past under these ideologically motivated prohibitions.
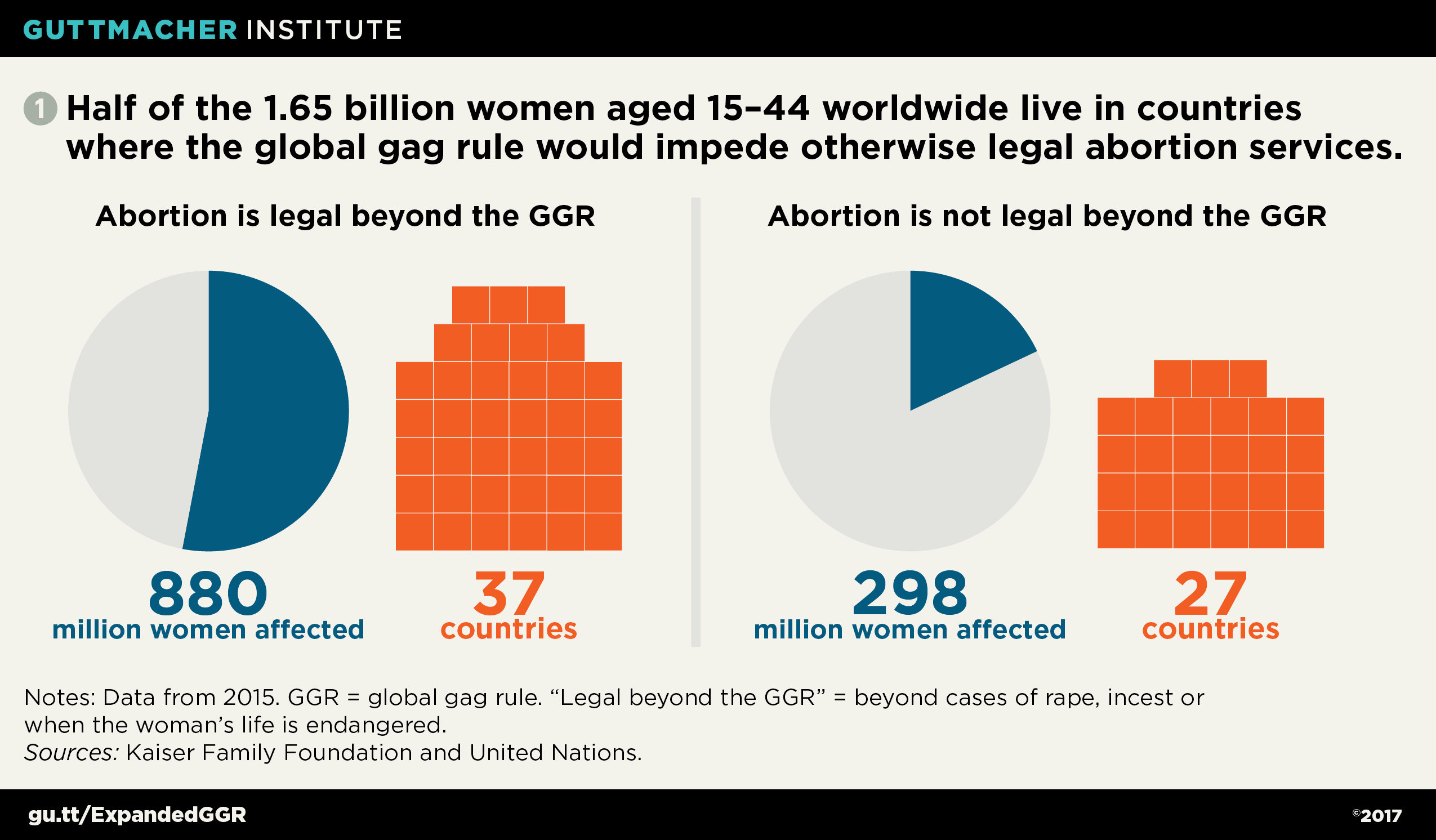
Several global health trends will exacerbate the impact of the expanded gag rule. First, the trend toward integrated health programs or co-located health services in low-income settings means that NGOs often offer an array of services to patients—such as contraceptive care, HIV prevention or treatment, prenatal check-ups, immunizations, and information or referrals on safe abortion care—all in one facility. Under the Trump global gag rule, these NGOs would be denied any global health funding from the United States because they provide integrated care that includes information or services related to abortion with non-U.S. funding. Second, as part of a movement to build capacity of local institutions, funding from USAID that used to flow to U.S.-based NGOs, which are exempt from the gag rule, has been moving toward local, spin-off NGOs, which must comply with the gag rule. Finally, the global trend toward liberalization of abortion laws means that there are more countries where access to legal abortion services will now be impeded by the gag rule. Among the 64 countries that received U.S. bilateral assistance for global health programs in 2016, 37 have laws allowing for abortion beyond the limited exceptions permitted under the gag rule (cases of rape or incest, or complications that threaten the life of the pregnant woman). Therefore, service providers in those countries would be unable to receive U.S. funding and also provide the full range of legally permissible abortion services (see chart 1).5,6
One likely effect of the expanded gag rule is that it would greatly disrupt continuity of care at the systemic, organizational and individual levels. U.S.-based organizations often partner with local NGOs to implement health care programs. The global gag rule would effectively undo many of these partnerships, leaving U.S.-based NGOs without significant local capacity and many women without another place to go for services. Indeed, this is why the United States generally invests its foreign aid in countries without strong health systems. In the end, U.S.-based organizations may simply be unable to find effective alternative partners to provide health services. Years of investment in building partnerships and efficient service delivery would disintegrate.
Those who advocate for patient-centered care understand this reality. For example, a patient and her children who receive HIV treatment from a facility that does not provide abortion services may also need other types of health care—such as maternal care, nutrition support, malaria treatment or reproductive health services—from clinics that do provide referrals or services for abortion. Requiring those clinics to withhold abortion-related services from this patient will not ensure her long-term health and well-being; it may force a desperate woman into a clandestine and unsafe procedure, leaving her potentially injured or dead. Removing U.S. funding from clinics could also lead to reductions in the range and capacity of their services to patients. In either case, patients will suffer. Ultimately, the global gag rule will lead to more expensive, less effective and less efficient health care delivery.
The global gag rule increases the risk of unintended pregnancies and unsafe abortions. Even when the gag rule was applied solely to family planning funding under previous U.S. administrations, the results of this policy were clear and devastating: In developing countries, it crippled family planning programs and the communities that they served.
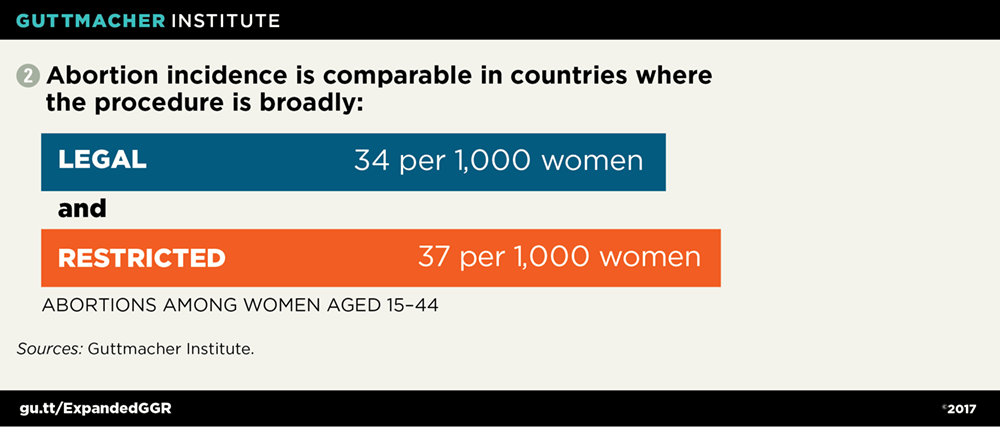
Contrary to what its proponents allege, the gag rule—like other restrictive abortion policies—does not stop women from seeking abortions (see chart 2).7 Rather, it reduces women’s access to high-quality contraceptive services, which in turn increases the probability of having an unintended pregnancy and seeking an abortion. Abortion is often unsafe in developing countries, and unsafe abortion is a major cause of maternal morbidity and mortality. In developing regions, 6.9 million women were treated for complications from unsafe abortion in 2012.8 More than 22,000 women die every year because of unsafe abortion, almost all of them in developing countries.
The global gag rule bans the most effective and trusted providers of family planning services from receiving U.S. aid if they refuse to abide by it. Providers face an untenable choice: provide contraceptives but give up their ability to provide legal and life-saving abortion services, including counseling and referrals, or face potentially drastic funding cuts in order to maintain their principled commitment to offering comprehensive reproductive health care. In the latter case, previous experience has shown that providers that were cut off from U.S. assistance by the global gag rule were forced to reduce their services, fire staff and sometimes close clinics.9 The ultimate irony is that—by undermining access to family planning services and denying women the tools they need to prevent unwanted pregnancies—the gag rule contributes to the very thing it purportedly seeks to reduce: the likelihood of abortion.
The global gag rule violates fundamental principles of medical ethics. In the United States, as in other countries, legal obligations and professional codes of ethics govern health care professionals and the care that they deliver to their patients. These codes and responsibilities generally contain a set of core values that require the provider to act in the best interest of the patient and her welfare. These guidelines support patients’ right to receive adequate, accurate and unbiased information that enables them to understand their options, provide informed consent to care and receive referrals so they are not effectively abandoned by the health care system.
For example, the World Health Organization offers technical and policy guidelines on the provision of safe abortion care that highlight these ethical standards in the provision of information and counseling for patients. With respect to abortion, they prescribe: "Information must be complete, accurate and easy to understand, and be given in a way that facilitates a woman being able to freely give her fully informed consent….States should refrain from limiting access to means of maintaining sexual and reproductive health, including censoring, withholding or intentionally misrepresenting health-related information."10 Similarly, the World Medical Association (WMA)—which provides guidance to physicians, national medical associations and governments around the world—insists that patients be given the information they need to provide informed consent to care and that patients have continuity of care, even when providers do not offer needed services.11 A specific WMA declaration on abortion makes it clear: "If the physician’s convictions do not allow him or her to advise or perform an abortion, he or she may withdraw while ensuring the continuity of medical care by a qualified colleague."12
Yet, the global gag rule directs providers to withhold information about a patient’s reproductive health options and bars providers from offering abortion referrals, violating the most basic standards of medical ethics. In countries where the procedure is legally permitted, providers have a duty to ensure that patients have information on all legal options and referrals to safe abortion services if needed or desired. Notably, even in countries where abortion is highly restricted, providers are obligated to act in their patients’ best interests and ensure that patients have timely access to safe abortion to the full extent of the law.
The global gag rule repudiates and undermines democratic values. Not only does the global gag rule muzzle health care professionals in a clinical setting, it suppresses the speech and political participation of non-U.S. actors in their own countries in coercive and hypocritical ways. In particular, it handcuffs organizations and advocates that would otherwise use their own funds to lobby their own government to legalize abortion (for reasons other than to save the life of the woman or in cases of rape or incest) and prohibits them from engaging in activities such as public information campaigns that educate citizens on the "benefits and/or availability" of abortion. Moreover, it gives a distinct advantage to antiabortion advocates in public debates on the issue, by not imposing the same limitations on those who aim to restrict abortion.
The rights to freedom of speech, expression and opinion are enshrined in many international and domestic laws worldwide. The Universal Declaration of Human Rights and the International Covenant on Civil and Political Rights guarantee these fundamental human rights, as does the First Amendment to the U.S. Constitution. Free speech is a core democratic principle championed by the United States, whether at home or through foreign aid, that supports the rule of law and good governance and democracy programs. As with other aspects of the global gag rule, this policy subverts the very goals of overall U.S. foreign policy.
The global gag rule must be repealed. Looking ahead, global health advocates will be seeking opportunities to mitigate the impact of this harsh policy. As has been done previously through federal agency guidance, the Trump administration has maintained the U.S. government’s long-standing support of postabortion care internationally for women who face complications from an unsafe abortion and will allow exceptions for abortions to be performed in cases in which a woman experiences rape, incest or a life-threatening pregnancy, as found throughout domestic antiabortion restrictions.
Meanwhile, advocates of global health who have never faced such a policy tried and failed to secure exemptions for those global health issues that are newly restricted under the gag rule. Notably, the Trump administration specifically included the President’s Emergency Plan for AIDS Relief (PEPFAR) under the gag rule—unlike the Bush administration, which exempted PEPFAR when it was authorized in 2003.13 Secretary of State Rex Tillerson has authority under the expanded gag rule to provide limited exemptions, but details are not yet available. While such carve-outs would help to mitigate the gag rule’s reach and impact, they would not change the underlying reasons such a policy is so harmful in the first place.
Ultimately, the only responsible and ethical response to this policy is full repeal. Champions of women’s health and global development in Congress—led by Sen. Jeanne Shaheen (D-NH) and Rep. Nita Lowey (D-NY)—have introduced the Global Health, Empowerment and Rights (HER) Act to legislatively rescind the global gag rule.
After decades of isolating and stigmatizing women’s legitimate reproductive health needs for abortion services from other "acceptable" health services, policymakers, providers and public health advocates now have to grapple with a Trump global gag rule that is the logical extension of an extremist, ideologically driven agenda. It should serve as a wake-up call to the entire global health community that avoiding, shunning or otherwise segregating abortion care to appease social conservatives can only lead down this road.