This publication has been updated, please see here for the latest version.
The proportion of women of reproductive age (15–44) who were uninsured dropped by 41% between 2013 and 2016, over the first three years of the Affordable Care Act’s (ACA) major expansions to Medicaid and private insurance coverage. This considerable decline in the uninsured rate, calculated by the Guttmacher Institute using data from the U.S. Census Bureau’s American Community Survey, mirrors broader national insurance trends, and was particularly pronounced in states that had expanded Medicaid under the ACA. These gains are now endangered, as conservatives in the Trump administration and Congress are determined to repeal the ACA and slash investments in affordable insurance coverage.

Overall, the proportion of reproductive-age women without health insurance fell from about 20% (12.5 million women) in 2013 to 12% (7.4 million) in 2016. The change was driven by substantial gains in both Medicaid coverage and private insurance. Medicaid, the federal-state health insurance plan for low-income individuals and families, covered 21% of reproductive-age women in 2016 (13.2 million).
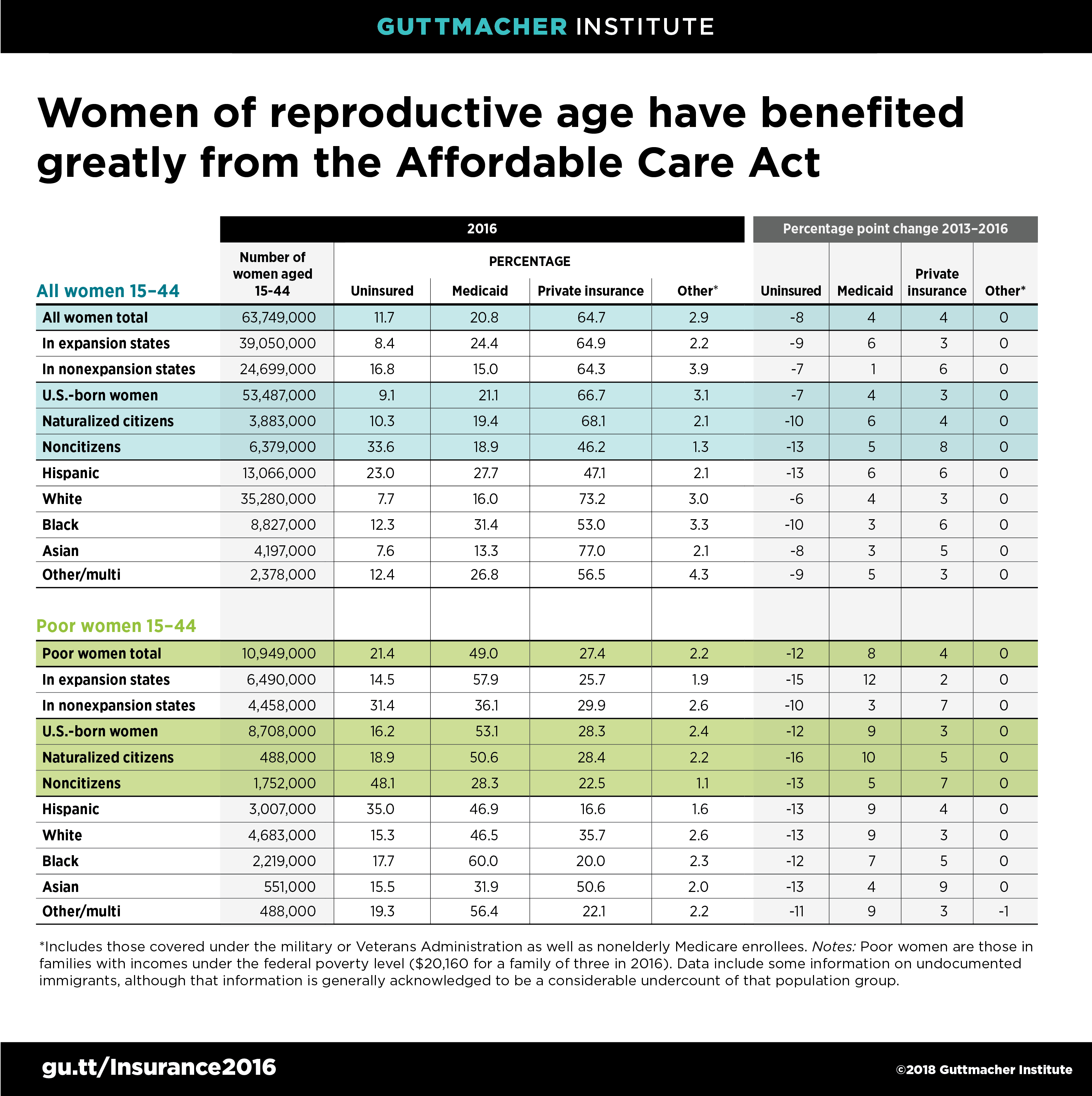
Gains in insurance coverage among reproductive-age women who live below the poverty line were substantial as well, with a 37% drop in the proportion who were uninsured and a 20% increase in the proportion covered by Medicaid. That program covered about half of women aged 15–44 with incomes at or below the federal poverty level in 2016. Despite these overall improvements, women of reproductive age who live in poverty were almost twice as likely to be uninsured in 2016 as reproductive-age women overall.
Other disparities in coverage also persist. Hispanic women of reproductive age were far more likely than white or black women to be uninsured in 2016. Similarly, immigrant women of reproductive age who are not citizens had close to four times the uninsured rate of U.S.-born women in 2016. That gap grew wider between 2013 and 2016, likely because many immigrants are barred from eligibility for subsidized private coverage under the ACA and for Medicaid coverage. In fact, nearly half of noncitizen immigrant women aged 15–44 living at or below the poverty level remained uninsured in 2016.

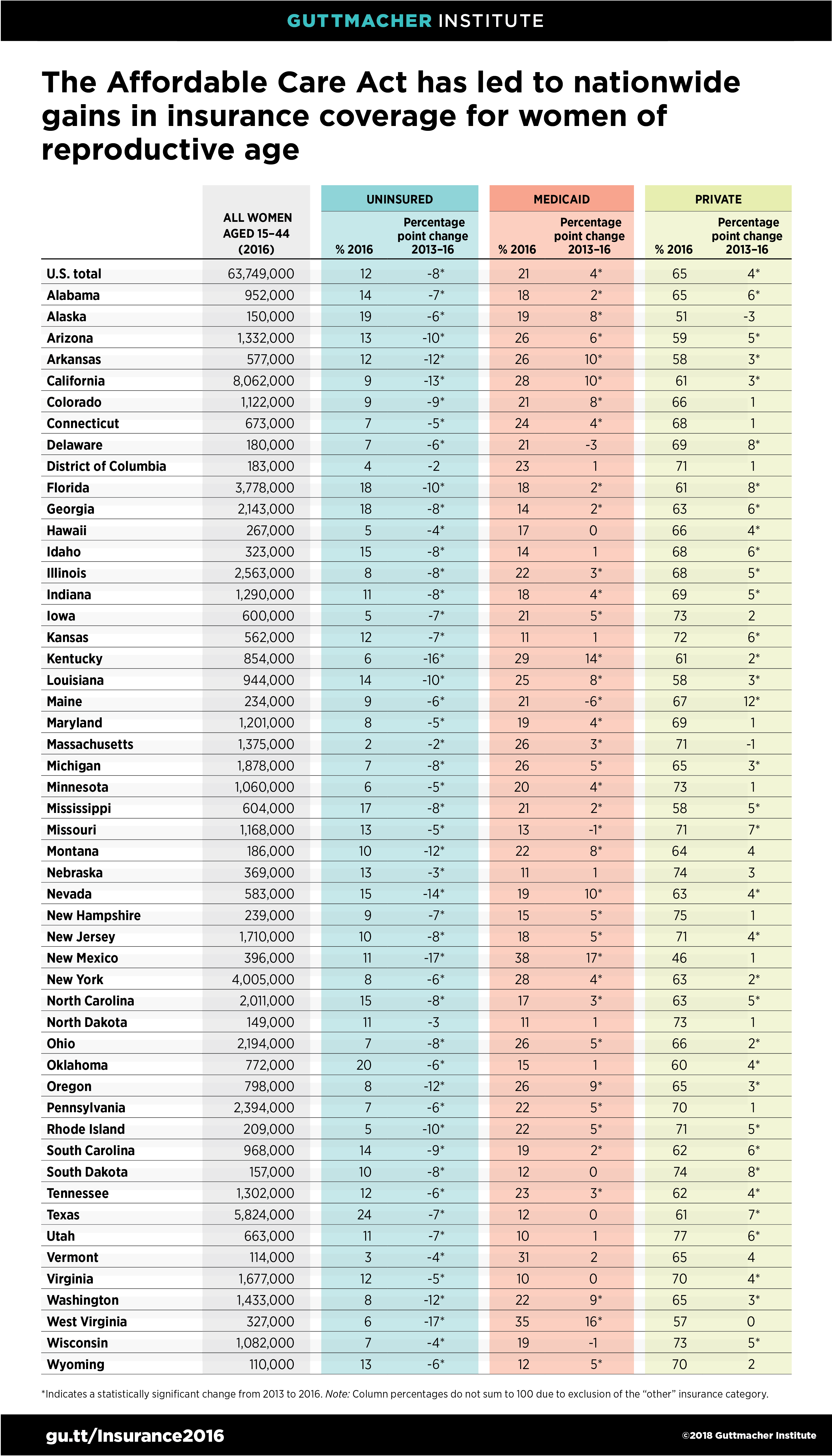
At the state level, improvements in insurance coverage across the country are tied to the ACA’s coverage expansions, particularly the major Medicaid expansion now adopted by 32 states and the District of Columbia. The uninsured rate declined significantly in almost every state in the country between 2013 and 2016. Collectively, states that implemented the ACA’s Medicaid expansion experienced steeper declines than nonexpansion states and had one-half the uninsured rate in 2016 (8% vs. 17%).
These gains in insurance coverage have major implications for access to health care in general and to sexual and reproductive health care in particular. That is because Medicaid and private insurance include robust coverage for many sexual and reproductive health care services, including family planning services and supplies and maternity care. In fact, Medicaid accounts for three-quarters of all public dollars spent on family planning in the United States and covers half of all U.S. births.
Alarmingly, conservatives in Congress spent much of 2017 trying to dismantle the ACA and reverse these gains in coverage. Although their full-scale repeal attempts have so far failed, Congress has repealed key pieces of the ACA, including the requirement that individuals maintain health coverage or else pay a tax penalty (a provision designed to stabilize the private insurance market and tamp down premiums).
The Trump administration has also worked on multiple fronts to undermine the ACA broadly and reproductive health coverage in particular, including by granting sweeping new authority for employers and universities to deny contraceptive coverage for employees, dependents and students. The administration is also working to reshape Medicaid in ways that would undermine its role as basic health insurance coverage, such as by establishing work requirements for many potential enrollees. Meanwhile, Congress and the Trump administration have also repeatedly attacked many of the safety-net family planning providers that both insured and uninsured people rely on for their care, and that will be needed even more if gains in insurance coverage are reversed.
State policymakers have the power to mitigate some of the potential damage and even to expand coverage for reproductive health services. For example, nine states over the past few years have adopted new requirements for private insurance plans to cover contraceptive methods and services without patient out-of-pocket costs—a move that mirrors the federal contraceptive coverage guarantee and protects against a rollback by the Trump administration. Similarly, states could protect against potential Trump administration actions to undermine Medicaid’s coverage of reproductive health care by establishing strong state-level coverage protections.
Even with these positive actions taken in some states, members of Congress who recognize the value of health coverage overall and reproductive health coverage specifically must continue to fight attempts to repeal or otherwise undermine the ACA and Medicaid. Health insurance coverage—provided by both private plans and publicly funded programs—is critical to enabling women to avoid unwanted childbearing and have healthy pregnancies and births when they so desire, and to addressing persistent reproductive health disparities in the United States.