In 2019–2020, women in Wisconsin aged 18–44 most preferred to get contraceptives in-person from a provider (69%), from a pharmacy (67%) and via telehealth (58%) for pick-up or home delivery. Across three states (Arizona, New Jersey and Wisconsin), 73% of women of reproductive age preferred more than one source for contraceptives.
What Family Planning Policies Changed in Wisconsin During the Study Period?
State and federal policy changes enacted during the RHIS study period disrupted the publicly supported reproductive health care system in Wisconsin. Planned Parenthood of Wisconsin had long been the state’s sole Title X grantee. In 2018, a Wisconsin state law went into effect, requiring the Wisconsin Department of Health Services (DHS) to apply for Title X funding. The law further required Wisconsin DHS to prioritize distributing Title X funds to public organizations and prohibited them from distributing these funds to agencies that provide abortions or are affiliated with organizations that provide abortions. Since 2019, Wisconsin DHS has been the state’s sole Title X grantee.
In 2019, the Trump-Pence administration implemented a series of changes to the Title X program’s administrative regulations that included a ban on abortion referrals, required physical and financial separation of Title X–funded activities from any related to abortion, and mandated coercive counseling standards for pregnant patients. As a result of this “domestic gag rule,” all Planned Parenthood affiliates left the Title X network later that year, although Planned Parenthood of Wisconsin continued to offer family planning services via other funding streams. In March 2019, Wisconsin joined 20 other states in filing a lawsuit opposing the gag rule. In 2021, the Biden-Harris administration’s Title X rule went into effect, revoking the 2019 rule and restoring the Title X national family planning program.
Patients’ Experiences of Reproductive Health Care in Wisconsin
The restrictive state and federal policy changes enacted from 2017 to 2024 negatively impacted Wisconsin residents’ ability to access reproductive health care.
Barriers to Accessing Care
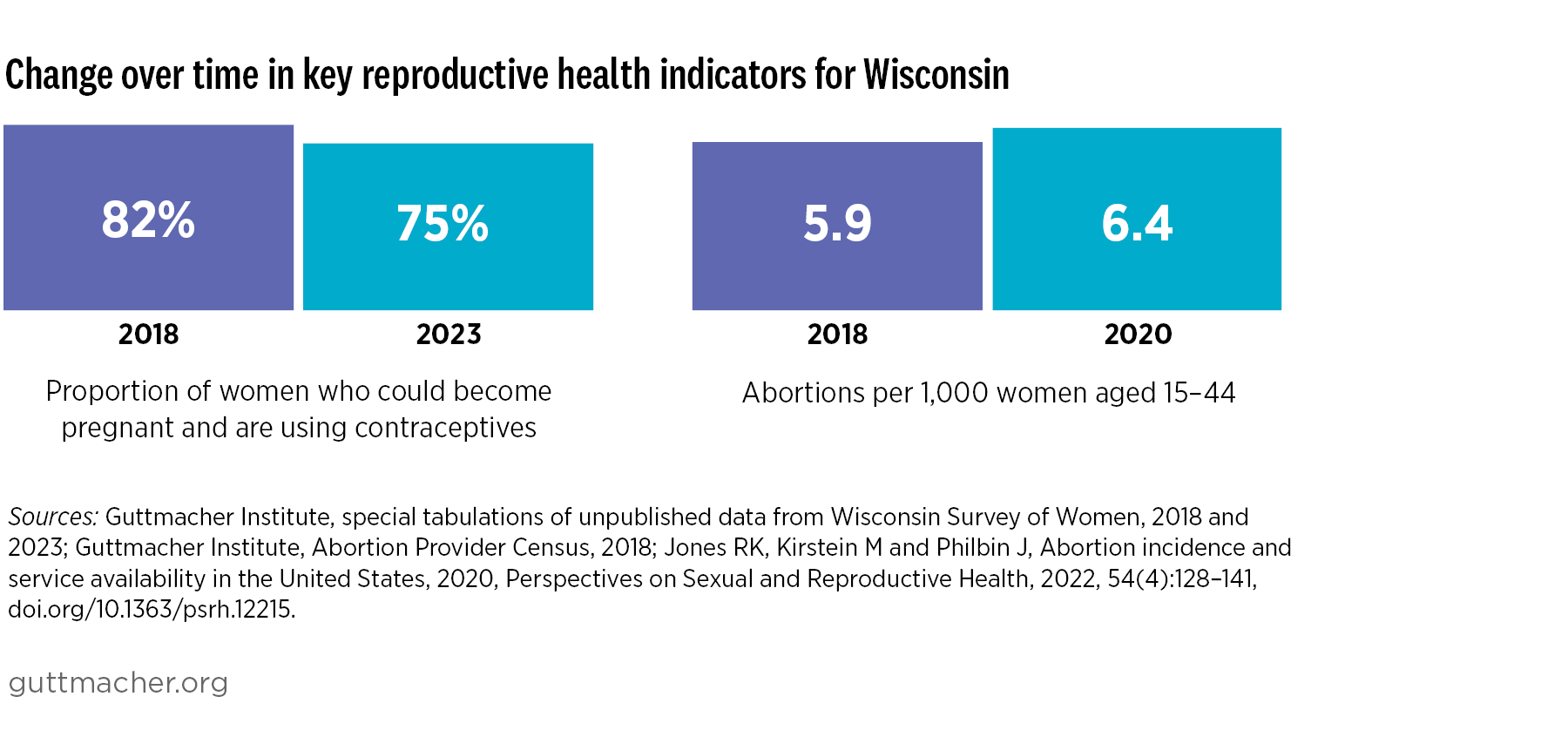
Restrictive state and federal policies undermine person-centered care, the patient-provider relationship and patient health outcomes. Person-centered care—health care responsive to an individual patient’s preferences and values—is a central tenet of reproductive autonomy. In 2019–2020, only about one-third (35%) of women aged 18–44 in Wisconsin reported receiving “excellent” person-centered contraceptive care in the previous year.3
Although state-specific data are not available, national findings indicate that restrictive sexual and reproductive policies compound existing inequities. Therefore, the effects of the policies implemented during the RHIS study period are likely to have fallen particularly hard on marginalized groups in Wisconsin, including communities of color, people with low incomes and immigrant communities.
Effects of COVID-19 and Dobbs on Care
The COVID-19 pandemic further exacerbated the harmful impact of restrictive sexual and reproductive health policies. Between May 2020 and May 2021, nearly one-third (30%) of survey respondents at publicly supported health centers in Wisconsin reported that they were unable to access or delayed accessing sexual and reproductive health care, including contraceptive care, because of the pandemic. Respondents who had experienced financial instability during the pandemic were more likely than those who had not to experience pandemic-related delays in accessing sexual and reproductive health care.
Abortion-related policy changes during the study period also impacted people’s ability to access contraceptive care. In 2022–2023, following the Dobbs decision that overturned Roe, 10% of reproductive-aged women in Wisconsin reported having trouble or delays in accessing their preferred contraception, compared to 6% in 2021.
Reproductive Health Care Providers’ Experiences in Wisconsin
Restrictive state and federal policies disrupt providers’ ability to center and meet patients’ needs. They also increase existing inequities in sexual and reproductive health care, because these policies disproportionately impact marginalized groups.
Barriers to Providing Care
The state and federal policy changes enacted during the RHIS study period hindered publicly funded family planning providers in Wisconsin from offering patient-centered care. They negatively impacted clinic finances, providers’ ability to protect patient confidentiality, contraceptive counseling and service provision, and pregnancy options counseling.
Providers at clinics that opted to join or stay in the Title X national family planning program after the gag rule was enacted were required to prioritize fertility awareness–based methods and include parents in care decisions for minors (potentially compromising patient confidentiality). In addition, they were no longer able to provide comprehensive pregnancy options counseling.
One Wisconsin provider reported: “We have to make sure that we're encouraging parental or guardian knowledge of contraceptive care and encourage them to talk with them, which has changed a lot, because previously, it wasn’t a concern because we are known as a confidential clinic, and in Wisconsin, they [were] able to seek those services without parental consent. It wasn't such a big deal, but now, adding that into our counseling has changed a little bit and figuring out that wording and making it sound appealing to the clients, especially those under 18, getting their parents involved. That's changed.”
Another provider shared: “As a family planning provider, it's our job to educate women on all of their options and when it comes to abortion, I feel like I'm swearing when I say it now.…it's become a curse word in Wisconsin.…When we talk to our patients, we still get young moms that come in here that don’t want to proceed with their pregnancy. They are 14, they are not going to have a baby. So, not being able to educate them on [abortion], and we don’t because of the gag rules that have been put in place, we have to be very mindful of what we do so we don’t lose funding.”
Changes in Title X Funding
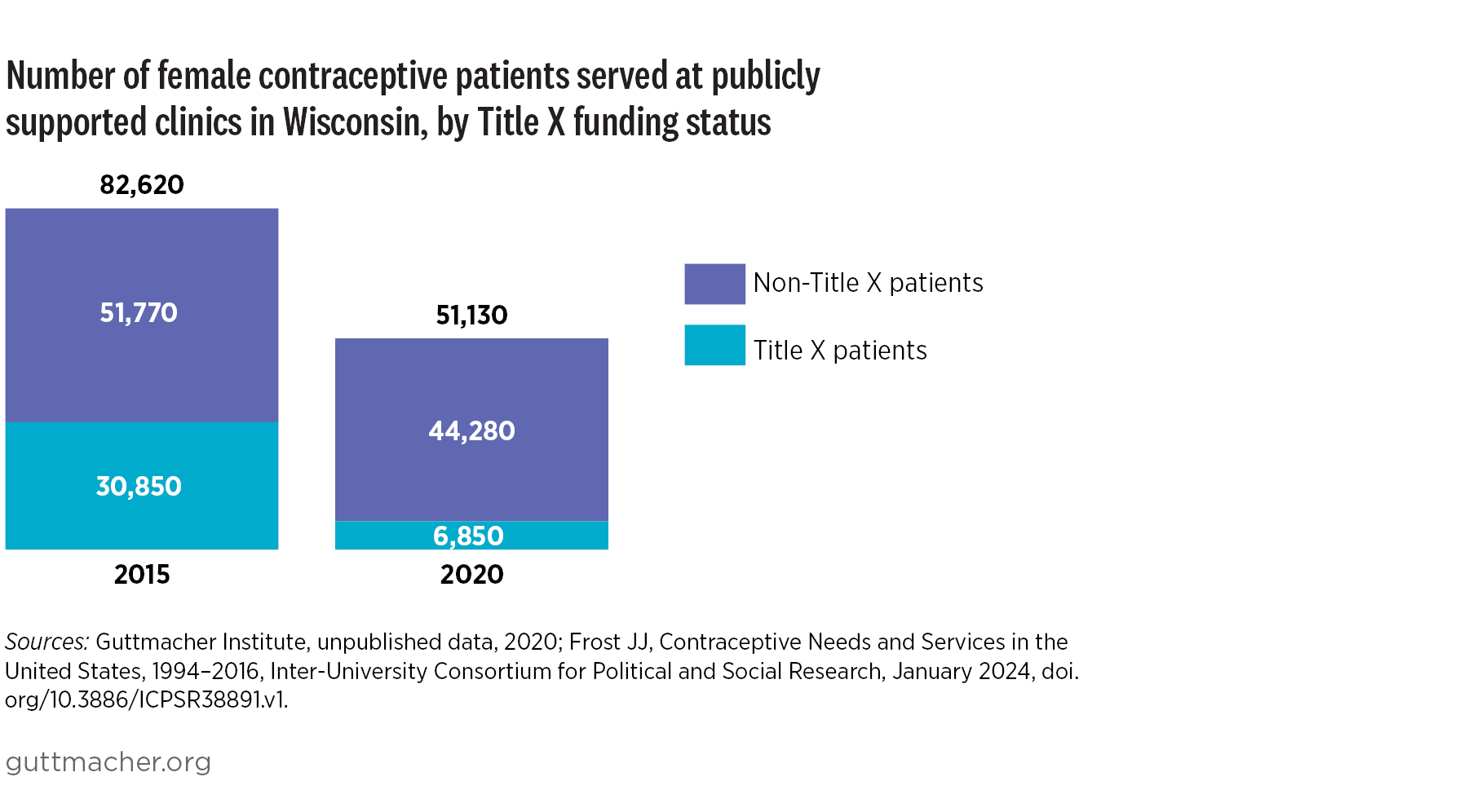
As a result of decreases or restrictions in funding, publicly funded family planning providers in all four RHIS study states—Arizona, Iowa, New Jersey and Wisconsin—had to rework payment options for patients. In some cases, they helped patients who would not otherwise be able to afford care access other government, clinic or donor funding sources.
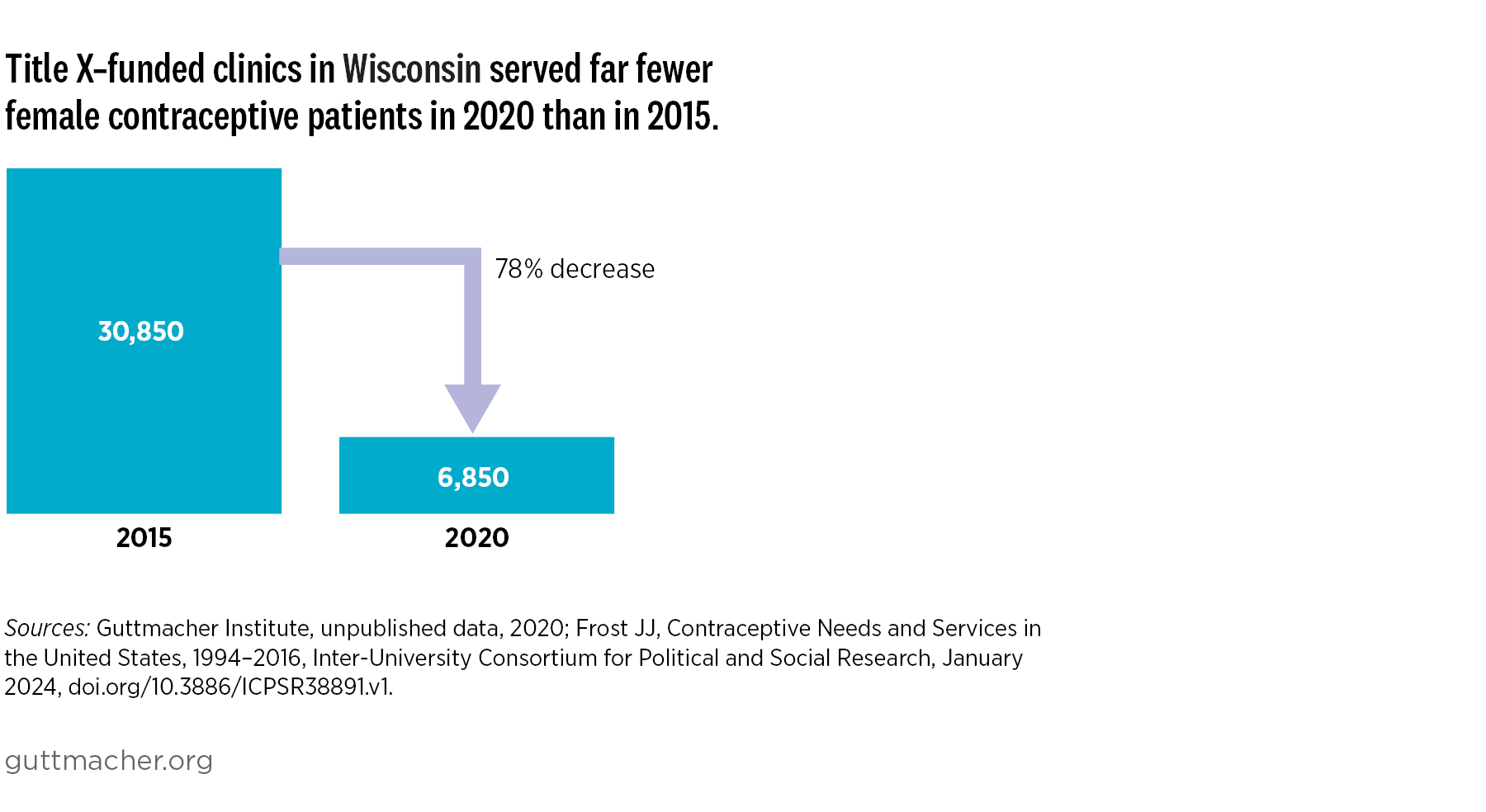
Between 2018 and 2021, 31% of publicly funded clinics in Wisconsin left the Title X family planning program, likely because of the gag rule. In the same period, the share of publicly funded clinics providing comprehensive contraceptive counseling decreased.
COVID-19 and Reproductive Health Care Provision
The COVID-19 pandemic further complicated Wisconsin providers’ ability to provide person-centered sexual and reproductive health care during the study period. Family planning providers adapted their operations—including by implementing additional safety protocols, shifting service delivery and staffing to meet patient needs, and expanding telehealth services—to continue providing care during the pandemic.
Wisconsin’s Post-Roe Abortion Policy Landscape
Restrictive abortion laws can affect people’s ability to access contraceptive services and family planning providers’ capacity to provide contraceptive and other sexual and reproductive health care. Whether or not a reproductive health care provider offers abortion services, the ripple effects of abortion policies impact all types of care.
After the Dobbs decision, all abortion clinics in Wisconsin stopped offering services while courts determined whether an 1849 state law criminalizing abortion was enforceable. As of 2024, Planned Parenthood of Wisconsin has resumed abortion services in three locations based on a county court ruling that the law did not prohibit voluntary abortions, and Affiliated Medical Services, an independent clinic in Milwaukee, has also resumed abortion services. The most current information about abortion-related policies in Wisconsin is available on Guttmacher’s interactive map of US state abortion policies.
State Partners
The Guttmacher Institute partnered with the
University of Wisconsin-Madison Collaborative for Reproductive Equity (UW CORE) and other Wisconsin-based research and policy partners for the RHIS. Additional information about reproductive health-related data and policies in Wisconsin can be found in the following resources:
NOTES
1. Throughout this profile, we use the terms female and women to refer to individuals who may have the ability to become pregnant. However, not everyone who has the capacity to become pregnant identifies as female or as a woman. A limitation of the data sources used in our analyses is that they do not provide further detail on the sex or gender identity of respondents.