Key Points
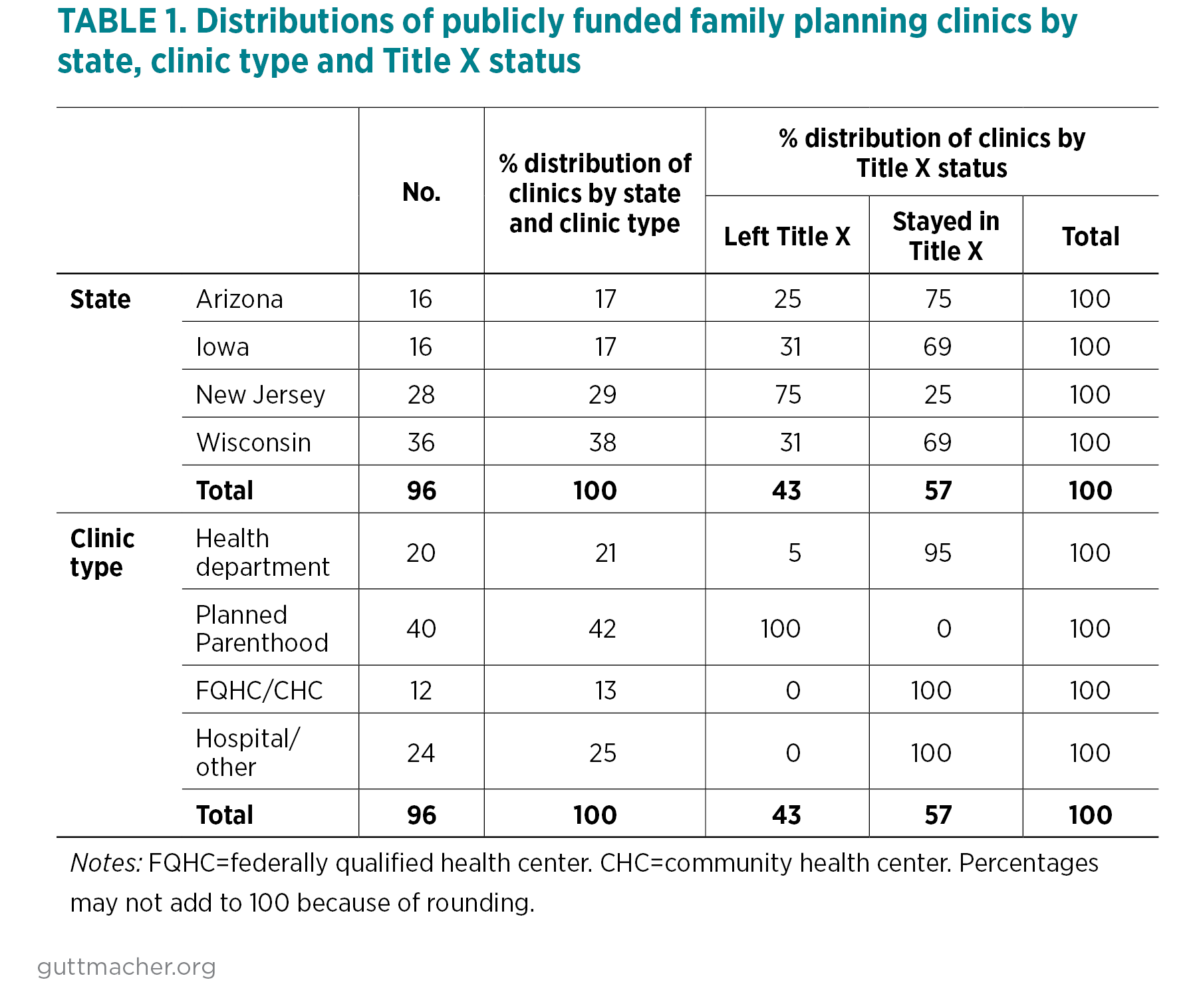
- Many of the publicly funded clinics in the four states studied in our sample left the Title X family planning program in 2018 because of a Trump-Pence administration rule that prohibited clinics from providing referrals for abortion care.
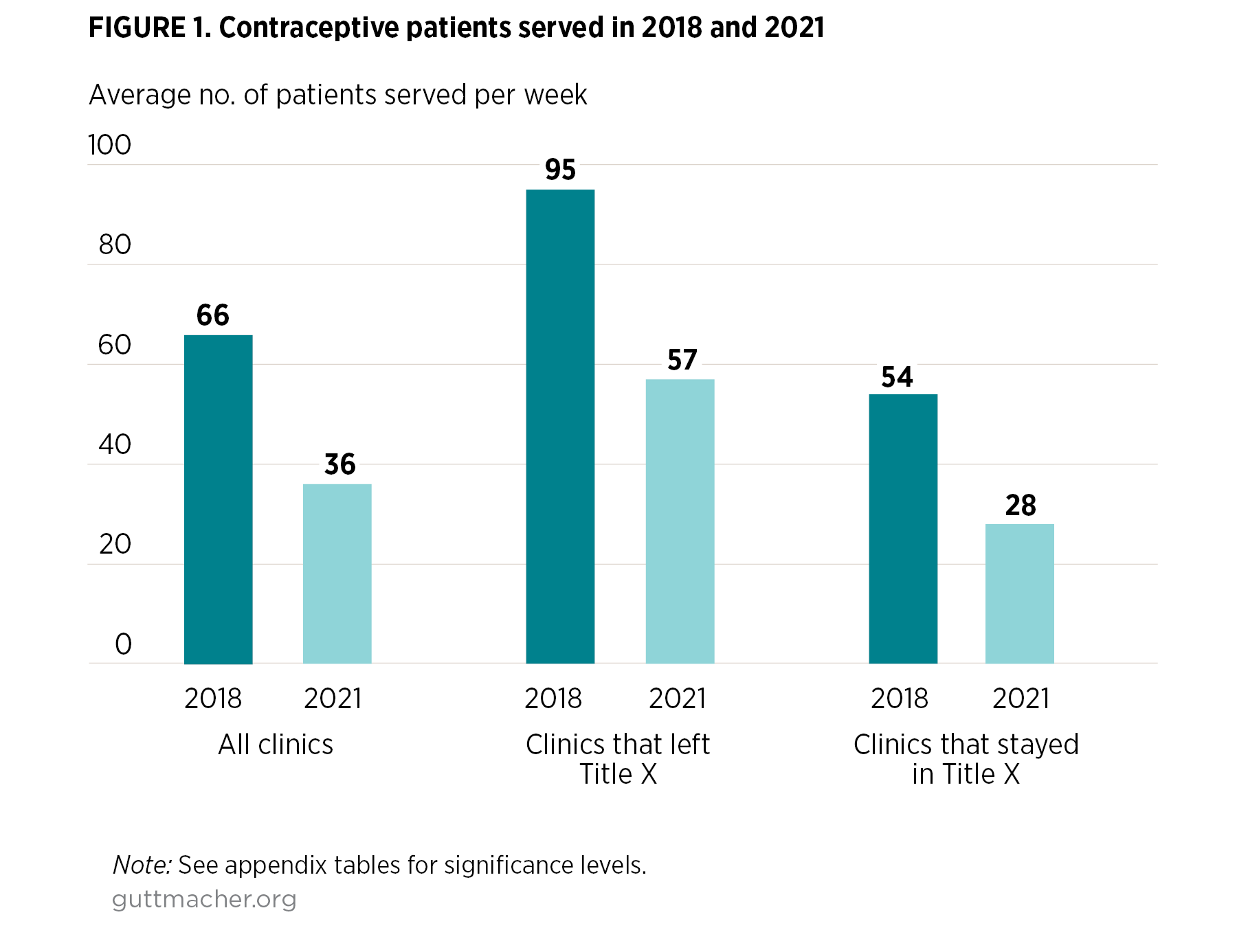
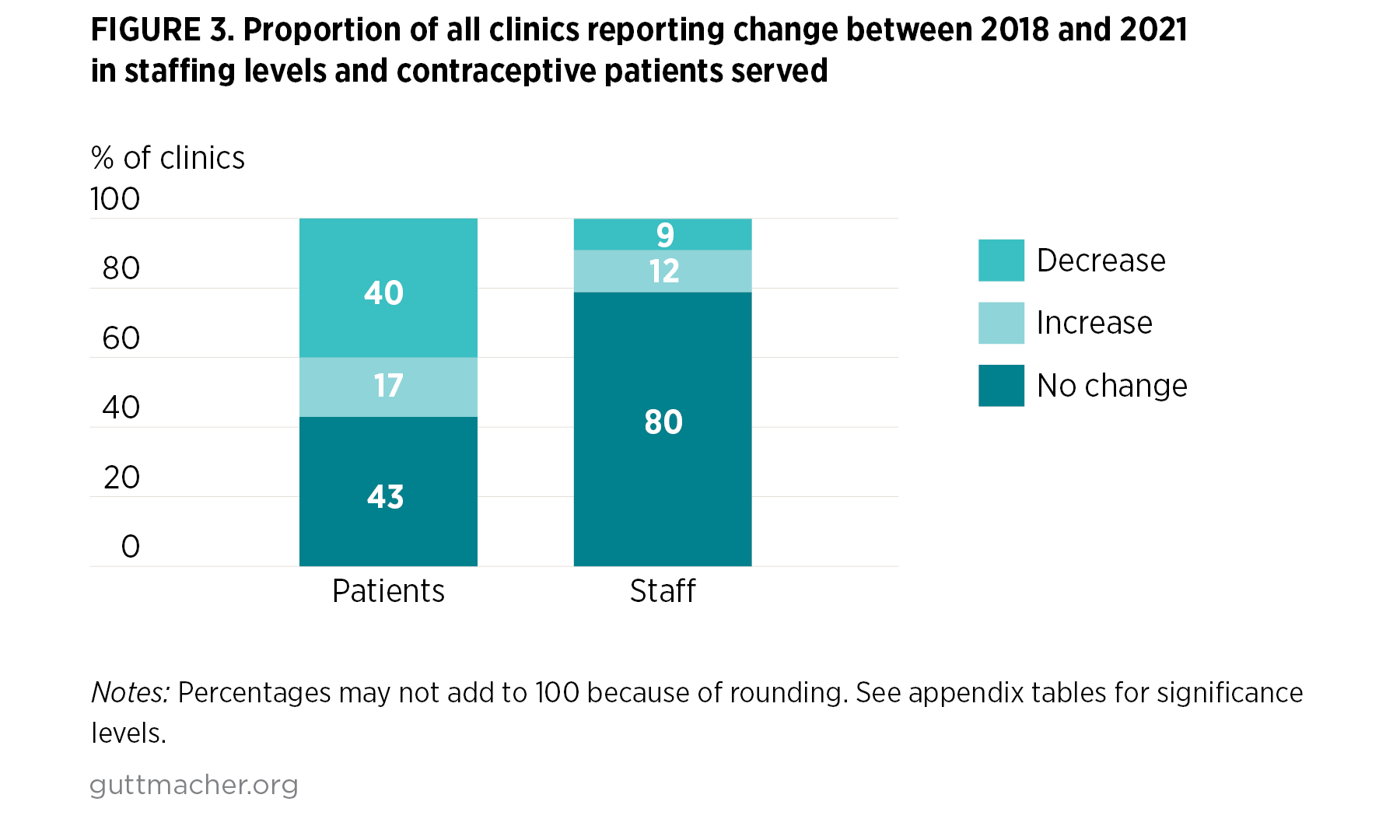
- The number of contraceptive patients served in publicly funded clinics in these four states declined between 2018 and 2021, most notably among sites that left the Title X program.
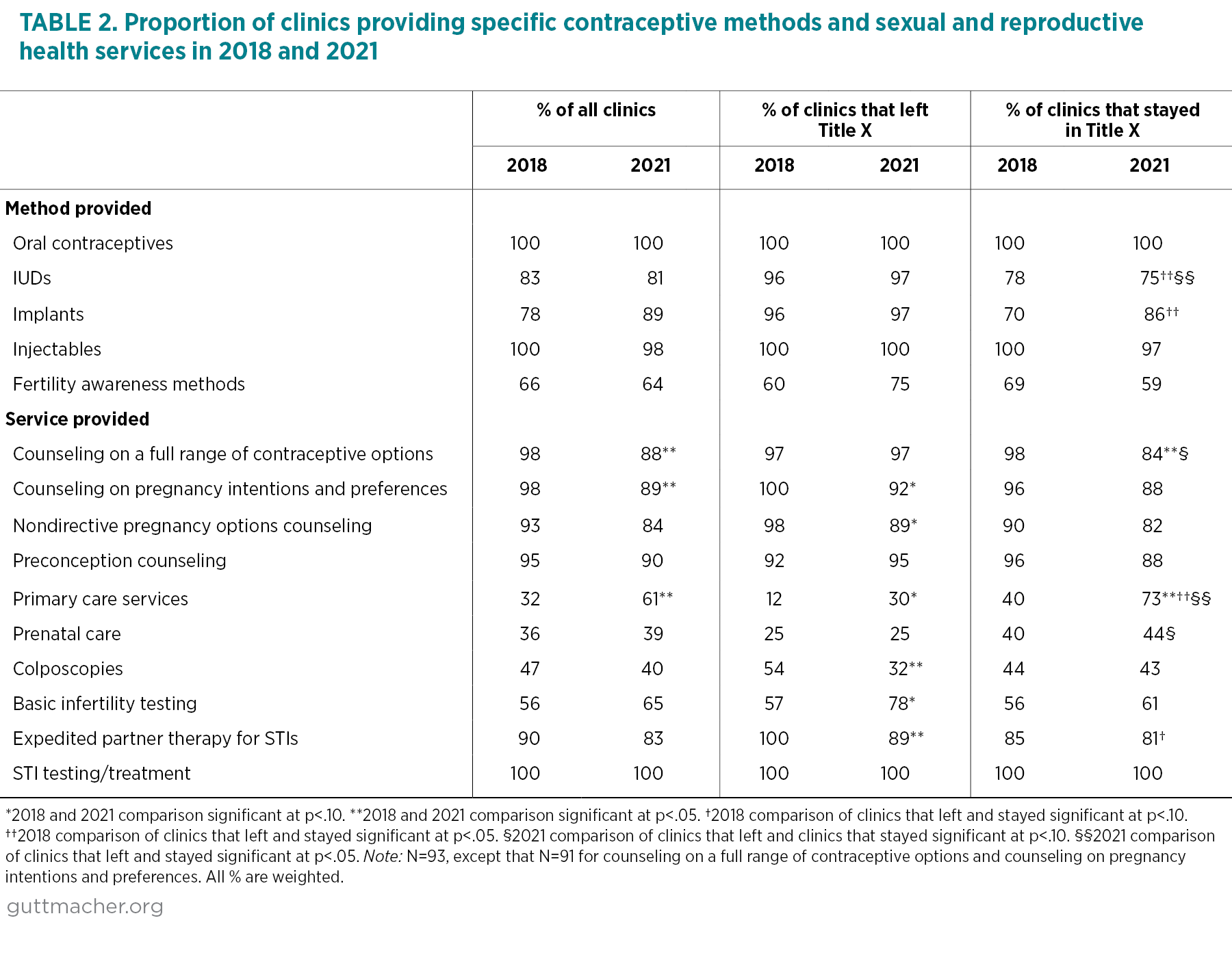
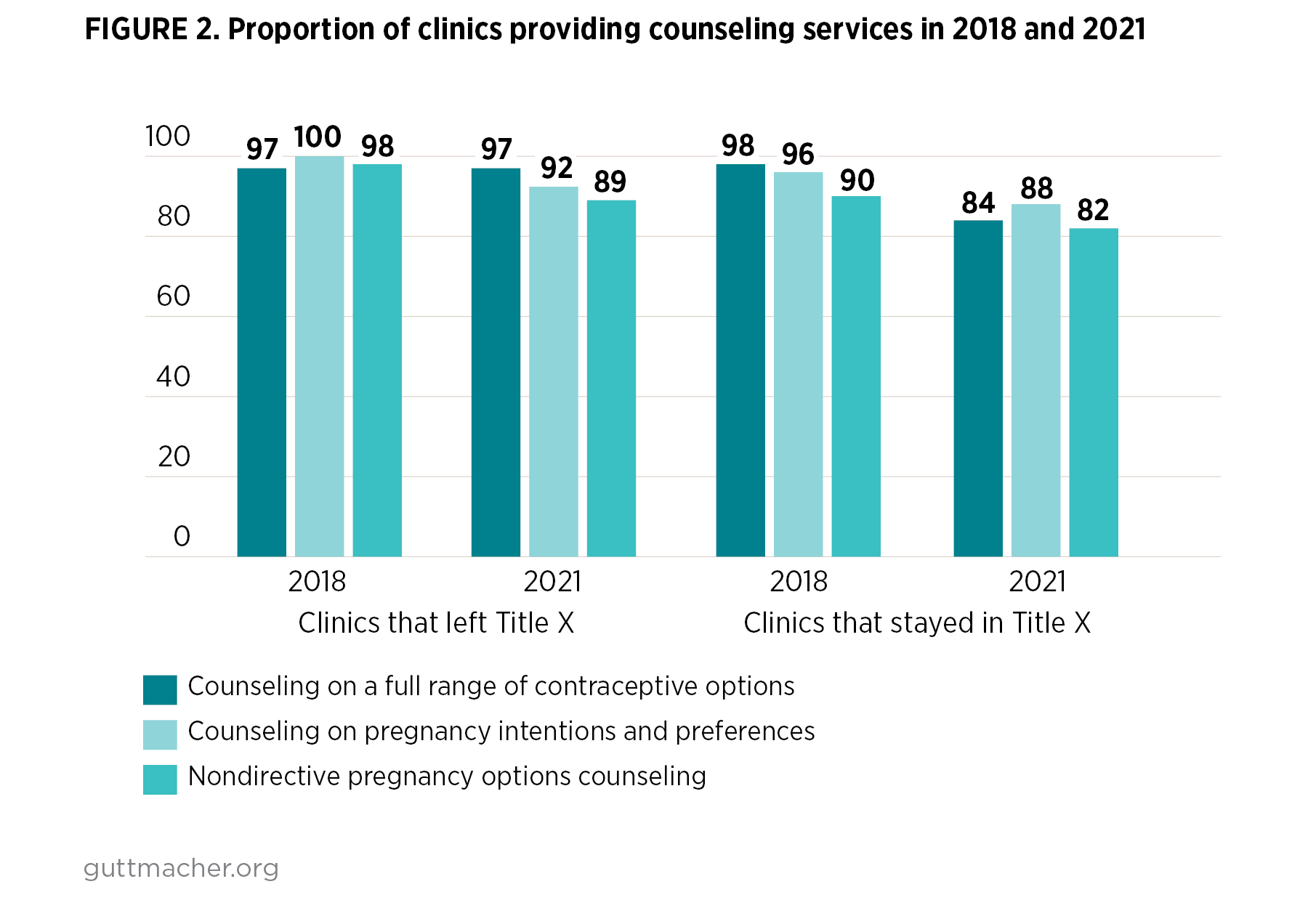
- Declines in the proportion of clinics that provided comprehensive contraceptive and pregnancy counseling were likely a result of the Trump administration’s Title X policies. For example, the proportion of clinics offering counseling on a full range of contraceptive methods fell between 2018 and 2021 among clinics that continued to receive Title X funding, while remaining high among sites that left the program.
- More clinics reported staff shortages and morale issues in 2021, following the onset of the COVID-19 pandemic, than in 2018.