Definitions and Terminology
In the Safe Abortion Calculator, induced abortions are classified as “safe,” “less safe” and “least safe,” based on the 2017 World Health Organization (WHO) definition of abortion safety.1 According to this definition, “safe” abortions are those provided by a trained provider, using an appropriate method for the pregnancy duration as recommended by the WHO. “Less safe” abortions are those that meet only one of the criteria for safe abortions, and “least safe” abortions are those that meet none of the criteria; the two types together form the category of “unsafe” abortions.
Safe abortion care, as defined in the calculator analysis, refers to the provision of abortion services that are supported fully or partially by the formal health care system, including access to accurate information, counseling and services. The current 2025 WHO abortion care guidelines2 also make clear that an abortion can be safely self-managed outside of a health care facility, provided an individual has access to accurate information, quality medicines and support from a trained health worker, if wanted or needed. While recognizing that people self-managing an abortion should have access to these services if they want or need them, the calculator does not include self-managed medication abortion in safe abortion care because of data scarcity to quantify incidence at the population level across low- and middle-income countries (LMICs).
Study Design
The Safe Abortion Calculator is based on a sub-analysis of Guttmacher Institute’s Adding it Up study. Adding It Up 2024 produced estimates on the need for, impact of and costs associated with providing sexual and reproductive health services in 128 LMICs.3 Adding It Up 2024 assesses the number of women of reproductive age (15–49) who need and receive contraceptive services, pregnancy-related and newborn services (including services for pregnant women and their newborns, safe abortion services and postabortion care), and treatment for the most common curable STIs. The project estimates total costs for providing care currently and estimates various hypothetical scenarios for increasing coverage for contraceptive care, pregnancy-related and newborn care, or both types of care together. This scenario-based approach facilitates comparisons between care as it is currently being provided and the associated costs and impacts of scaling up care to meet all needs for sexual and reproductive health services.
The Safe Abortion Calculator analysis adopts the analytic framework and core assumptions of Adding It Up as outlined in the Adding It Up 2024 Methodology Report,4 and introduces updated assumptions, data sources and analytic approaches that focus specifically on the abortion and postabortion care components. In addition, the calculator introduces a hypothetical scenario whereby safe abortion care provision is incrementally increased, to examine the associated impacts on abortion and postabortion care provision and costs. Table 1 provides information about the underlying data inputs and strength of the evidence for the various assumptions in this analysis.
Data Sources
The calculator generates estimates for a subset of the countries included in the Adding It Up 2024 analysis. Specifically, we only include LMICs in subregions where unsafe abortion is a persistent problem—defined as subregions with an estimated incidence of unsafe abortion above 25%.1 The analysis includes 117 countries across Africa, Asia, Latin America and the Caribbean, and Oceania. To estimate the total induced abortions by country for 2024, we leverage country-specific, model-based estimates of the annual number of abortions and the annual number of births in 2015–2019 in each country 5 to calculate a ratio of abortions to births. For countries without publicly available model-based abortion estimates, we use model-based subregional estimates of abortions due to a lack of country-level estimates. To generate country-specific abortion incidence for 2024, we apply the abortions-to-births ratio to the number of births in 2024 per World Population Prospects.6 We assume that all abortions occur among women experiencing unintended pregnancies.
We subdivide the total number of induced abortions in each country by safety based on the abortion safety definitions from Ganatra et al.1 For five countries where data are available, we use country-specific studies to classify abortions into safety categories;7–11 for the remaining 112 countries, we apply subregional estimates of safety from Ganatra et al. We then distribute abortions within safety categories by abortion method type. We determine these distributions primarily based on expert opinion, supplemented with medication abortion information available from Gynuity Health Projects12 and the Medical Abortion Commodities Database.13 Methods for safe abortion include manual or electric vacuum aspiration, dilation and evacuation, and medication abortion (either misoprostol only or both misoprostol and mifepristone). Methods for less safe abortion encompass manual or electric vacuum aspiration, dilation and curettage, and medication abortion (misoprostol or both misoprostol and mifepristone). We assume that least safe abortions occur entirely outside of the health care system; therefore, we do not estimate service provision and costs for such abortions and do not divide them by method.
Some induced abortions result in health outcomes that require medical care; the vast majority of abortion-related complications are due to unsafe abortion. To estimate the number of induced abortions resulting in complications, we apply a complication rate to safe and unsafe abortions. We assume one standardized safe abortion complication rate of 3% across all included countries, based on country-specific data available on abortion from Ethiopia and Nepal.8,14 We also assume one standardized unsafe abortion complication rate of 40%, based on prior abortion estimation that compiled data from several country-specific abortion studies that relied on the opinions of health professionals and others knowledgeable about abortion in their countries.15
Abortion complications are known to range in severity and symptomology. To estimate the proportion of abortion complications with specific severity and symptoms, we compiled data from several literature sources. Specifically, we extracted the underlying data from a 2018 systematic review, as well as additional abortion incidence studies, to generate postabortion care symptom distributions.16–44 Patients presenting with abortion complications may experience multiple complications at once; therefore, the categories are not mutually exclusive. We assume the same proportions of types of complications regardless of abortion safety, as there is a lack of evidence to otherwise inform our analysis. This assumption likely overestimates the severity of complications from safe abortions, given what we know from high-income countries about the safety and effectiveness of safe abortion care.45–49 Taking this conservative approach avoids underestimating the postabortion care costs associated with safe abortion cases. Across all types of abortions, an estimated 87% of complications are considered non-severe and an estimated 13% of complications are considered severe.
In this analysis, we estimate the costs associated with abortion care and postabortion care for all included countries. To do so, we estimate the direct costs (e.g., drugs, supplies, personnel time and inpatient hospital food) associated with induced abortion and postabortion care. For drugs and medical supplies, we consult a variety of procurement pricing resources to locate the most recent price for a specific item and assume the same cost across all countries due to limited data availability. For this analysis, we procure drug and supply costs from UNICEF,50 the IDA Foundation,51 UNFPA52 and other online sources.53–59 The Adding It Up 2024 Methodology Report4 outlines our approach for personnel costing data in detail. For this analysis, we follow the same inflation approach, with salaries adjusted to 2026. For hospital costs, we use an assumption for daily hospital food costs and adjust to 2026. We also estimate indirect costs, which are the costs of the programs and systems required to provide abortion and postabortion care. We combine the direct and indirect costs to estimate a total cost per case. For this analysis, costs are estimated in 2026 US dollars.
Analytic Framework
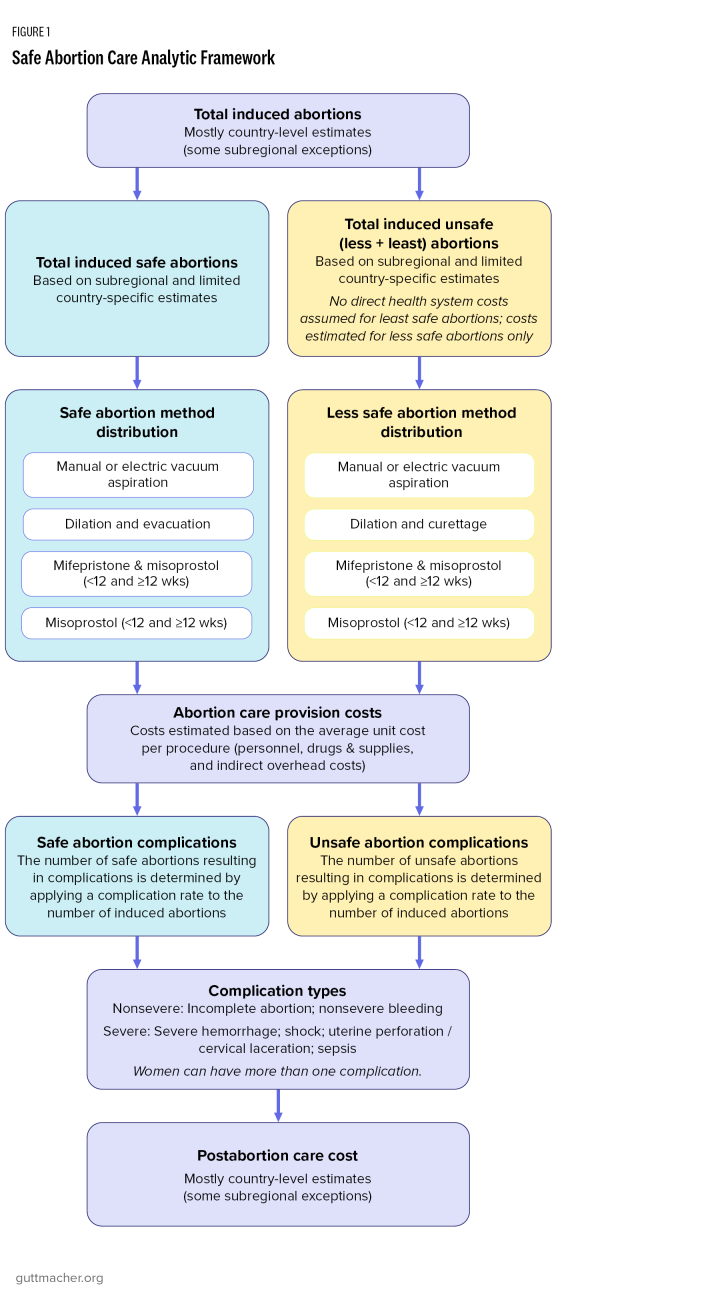
First, this analysis generates current estimates of abortion incidence by safety and postabortion care across the 117 included LMICs. For abortion services, we estimate the number of safe and unsafe abortions by estimating total induced abortions, dividing them into safety categories and distributing them among methods. For postabortion care for complications from induced abortion, we estimate the number of abortions resulting in complications based on the aforementioned abortion complication rates by safety. We assume that all complications are treated regardless of safety, though in many countries, women needing postabortion care may not receive it. For women requiring prereferral management of abortion complications, we assume that the number of women needing this intervention is equivalent to the proportion of women needing treatment in a comprehensive emergency obstetric facility who do not receive care in such a facility or receive no care. Further, we assume that the number of complications needing this intervention is equivalent to the proportion of deliveries not receiving care in comprehensive emergency obstetric facilities. Then, we calculate the costs of induced abortion and postabortion care services. Figure 1 outlines the analytic framework for this analysis.
Second, this study estimates the impacts of scaling up the provision of safe abortion care. To do so, the proportion of abortions that are classified as safe in a particular country is increased by 1% increments until 100% of abortions are safe. Each percentage increase in safe abortion care provision necessitates a 1% decrease in unsafe abortion care provision; in other words, unsafe abortions are reclassified from unsafe to safe incrementally and at each step, all components of the analysis are calculated—induced abortion care costs, the number of resulting postabortion care complications and postabortion care costs.
All analyses were conducted in Stata version 17.0.60