- According to the penal code of the Democratic Republic of Congo (DRC), abortion is prohibited without exception. Legal prohibition notwithstanding, it is generally accepted that the procedure can be performed to save a woman’s life; yet, women are rarely able to obtain safe abortion care on this basis. The vast majority of abortions occurring in the DRC are clandestine, and many of these are unsafe.
- The DRC is a signatory to the Maputo Protocol, a regional treaty on women’s rights that directs states to legalize abortion when necessary to protect a woman’s physical and mental health, as well as in cases of rape, incest and fetal anomaly.1 In March 2018, the government published the protocol in the nation’s legal gazette, officially entering the treaty into force.2
- The DRC’s maternal mortality rate—at 693 maternal deaths per 100,000 live births—is among the highest in the world, despite recent improvements. Unsafe abortion likely contributes substantially to this high rate of maternal deaths.
- Kinshasa is the DRC’s capital and largest urban area, and its population of 12 million accounts for 15% of the country’s total population. There is currently no reliable estimate of the incidence of abortion for the DRC as a whole, but the following new data are available for Kinshasa.
Incidence of abortion
- An estimated 146,700 abortions were performed in Kinshasa in 2016. This translates to an abortion rate of 56 per 1,000 women of reproductive age (15–49), which is much higher than the regional rate for Middle Africa overall (35 per 1,000 women in 2010–2014.)
- The abortion rate in the urban center of Kinshasa is likely higher than that for the country as a whole, given that a pattern of elevated rates in capital cities has been observed in other African countries where nationally representative studies have been conducted.
Provision of postabortion care
- Unsafe abortion is common in Kinshasa, and the level of postabortion care gives clues as to its prevalence and consequences. In 2016, an estimated 37,900 women obtained treatment in health facilities for abortion-related complications. These women represent only a portion of those who experienced an unsafe abortion: Some women encounter barriers that prevent them from obtaining needed postabortion care, while others do not require such care.
- Private hospitals and health centers, including those run by NGOs, treated 93% of all postabortion care patients in 2016. The remaining 7% of patients were treated in public-sector health facilities.
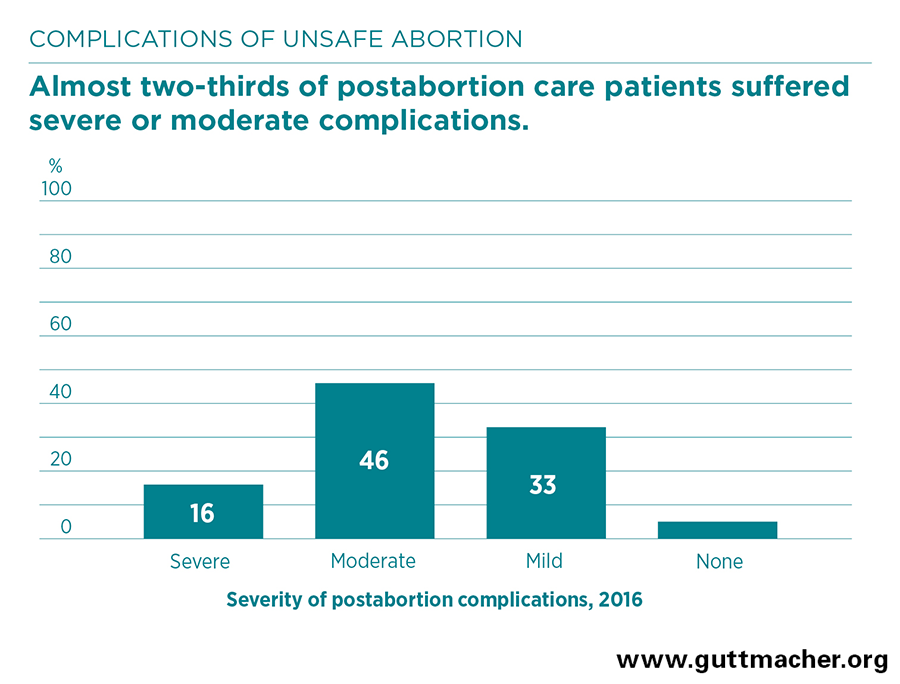
- Among women treated for postabortion complications, 16% experienced severe complications (such as shock, organ failure or death), 46% had moderate complications (such as localized infections) and 33% had mild complications (such as a low fever or prolonged bleeding). The remaining 5% who sought care did not require treatment. Just 15% of women with severe complications received pain medication as part of their postabortion care.
- Patients’ complications were most commonly treated using outdated methods, such as dilation and curettage (D&C), which is riskier and more invasive than vacuum aspiration and medication abortion, the methods recommended by the World Health Organization (WHO).3
- Contraceptive services to help prevent future unintended pregnancies is a critical part of postabortion care. Sixty percent of postabortion care patients in Kinshasa in 2016 received contraceptive counseling.
Patient characteristics and outcomes
- Most women presenting for postabortion care in 2016 had a secondary education or higher. About three-quarters had not had an abortion before, and 81% were in their first trimester when they terminated their pregnancy.
- Women’s health outcomes varied according to social and economic factors. Women who were single or cohabiting had nearly twice the odds of those who were formally married of experiencing severe or moderate complications, and poor women had higher odds of experiencing severe or moderate complications than nonpoor women.
Contraception and unintended pregnancy
- In Kinshasa, 72% of married women reported in 2017 that they wanted to delay or prevent having a child. However, only 23% of married women were using a modern method of contraception.4
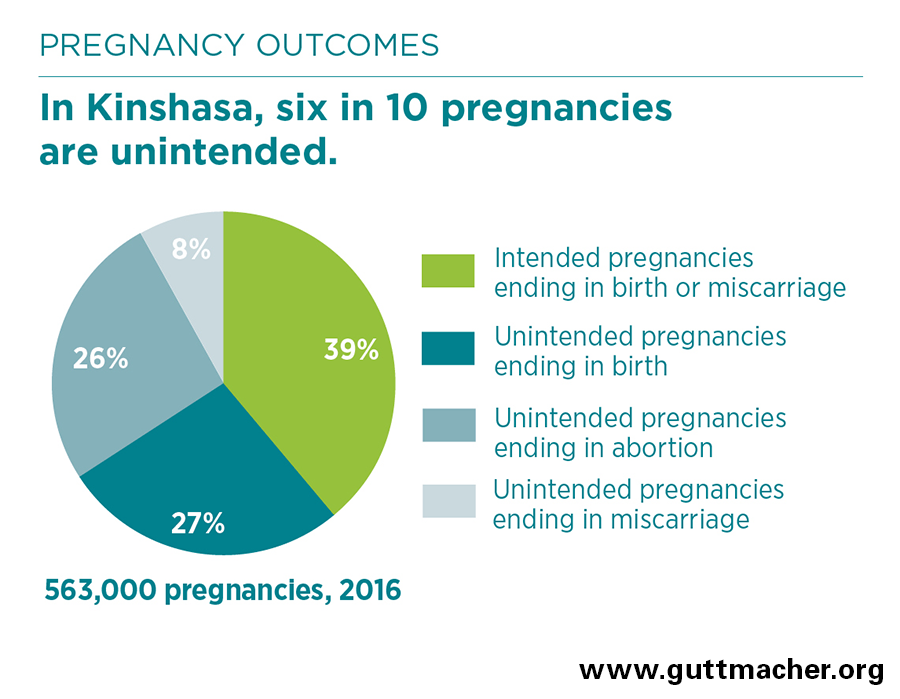
- In 2016, more than 343,000 unintended pregnancies occurred in Kinshasa, which translates to a rate of 147 unintended pregnancies per 1,000 women aged 15–49. Six in 10 pregnancies were unintended, and close to half of unintended pregnancies ended in abortion.
Recommendations
- Unsafe abortion poses a preventable threat to many women’s health and well-being, and it puts a significant strain on the DRC’s limited health care resources. Since most abortions occur in response to unintended pregnancy, greater efforts are needed to improve contraceptive services, including the counseling and information that would help women identify and adopt methods that best meet their needs.
- The Ministry of Health should draft and widely disseminate new standards and guidelines to reflect the expanded legal access to abortion implied by the government’s publication of the Maputo Protocol. To increase access to safe abortion services, investments must be made to educate health providers about the new provisions and train them to provide safe services using WHO-recommended methods, and public awareness must be raised about women’s right to such care.
- The quality of postabortion care must be improved. Health providers need training in best practices in order to provide high-quality postabortion care, and low provision of care by public facilities should be addressed by ensuring these facilities have the necessary equipment and supplies.
