Until recently, the vast majority of women of reproductive age in Latin America and the Caribbean, 97%, lived where abortion was highly or moderately restricted by law.1 That proportion fell when Argentina’s Law 27.610 went into effect in January 2021.2 However, passage of a law does not ensure full and equitable implementation; assessment is needed to identify successes and emerging challenges.
The new law allows abortions on request through 14 weeks of pregnancy, as well as after 14 weeks in cases where continuing the pregnancy threatens the pregnant person’s life, physical health or mental health, and in cases of rape. Modeled estimates suggest that in 2015–2019, some 33 abortions occurred each year per 1,000 women of reproductive age; these correspond to nearly half (48%) of all unintended pregnancies in the country,3 indicating that many Argentines are motivated to avoid taking unintended pregnancies to term.
This fact sheet summarizes key findings from a study of abortion service provision by public-sector facilities in three provinces of Argentina in approximately the first two years of implementation of the law. It also makes recommendations to improve abortion access throughout the country.
Background on the study
The Guttmacher Institute partnered with Centro de Estudios de Población (CENEP), a nonprofit research center in Argentina, to assess the early phase of implementation in the public sector. To obtain a range of perspectives, data were collected in four areas of three provinces. Two areas were in Buenos Aires province. The first of the two areas, Gran Buenos Aires (GBA), is made up of districts surrounding (but not including) the capital city, and the population has good access to health care and comparatively open attitudes toward abortion. The second area, the rest of Buenos Aires province, is more socially conservative and has more limited access to health services. The other two provinces were Chaco and La Rioja; these two provinces are far poorer, more rural and more socially conservative than Buenos Aires province.
Researchers conducted two surveys. This fact sheet summarizes the results of one of them (see Source below for the results of both surveys in Spanish). To gauge the availability and characteristics of abortion services, 223 public facilities were surveyed in September 2022–January 2023. Because respondents were asked to supply data on aspects of services provided in the past six months, the period covered encompasses March 2022–January 2023. Respondents represented a broad range of facility types—primary health centers, midlevel municipal (secondary-care) hospitals and province-level tertiary-care hospitals.
Abortion provision by facility type and area
- Overall, a majority of facilities surveyed were providing abortions. By facility type, 94% of municipal hospitals were providing abortions in the first two years of the law, as were 62% of health centers and 63% of province-level hospitals.
- In Buenos Aires province (both GBA and the rest of the province), where the sample of facilities was drawn from the government list of abortion providers, the vast majority—88%—of facilities surveyed were providing abortions. In La Rioja and Chaco* provinces, the sample was drawn from all facilities (since their abortion provision status was not known). Only 40% of facilities in La Rioja and 9% in Chaco were providing abortions.
- More than 90% of the abortions provided in the previous six months in municipal hospitals and health centers were on-request abortions (through the 14th week). The proportion performed on specified legal grounds after 14 weeks was substantial (24%) only in province-level (tertiary) hospitals, probably because these facilities are more likely than others to receive referrals of women seeking such abortions. Moreover, because province-level hospitals offering abortions after 14 weeks are concentrated in GBA, the proportion of all abortions that were after 14 weeks reached 10% in that area, but was far lower (0–4%) in the other three areas.
Most common method of abortion
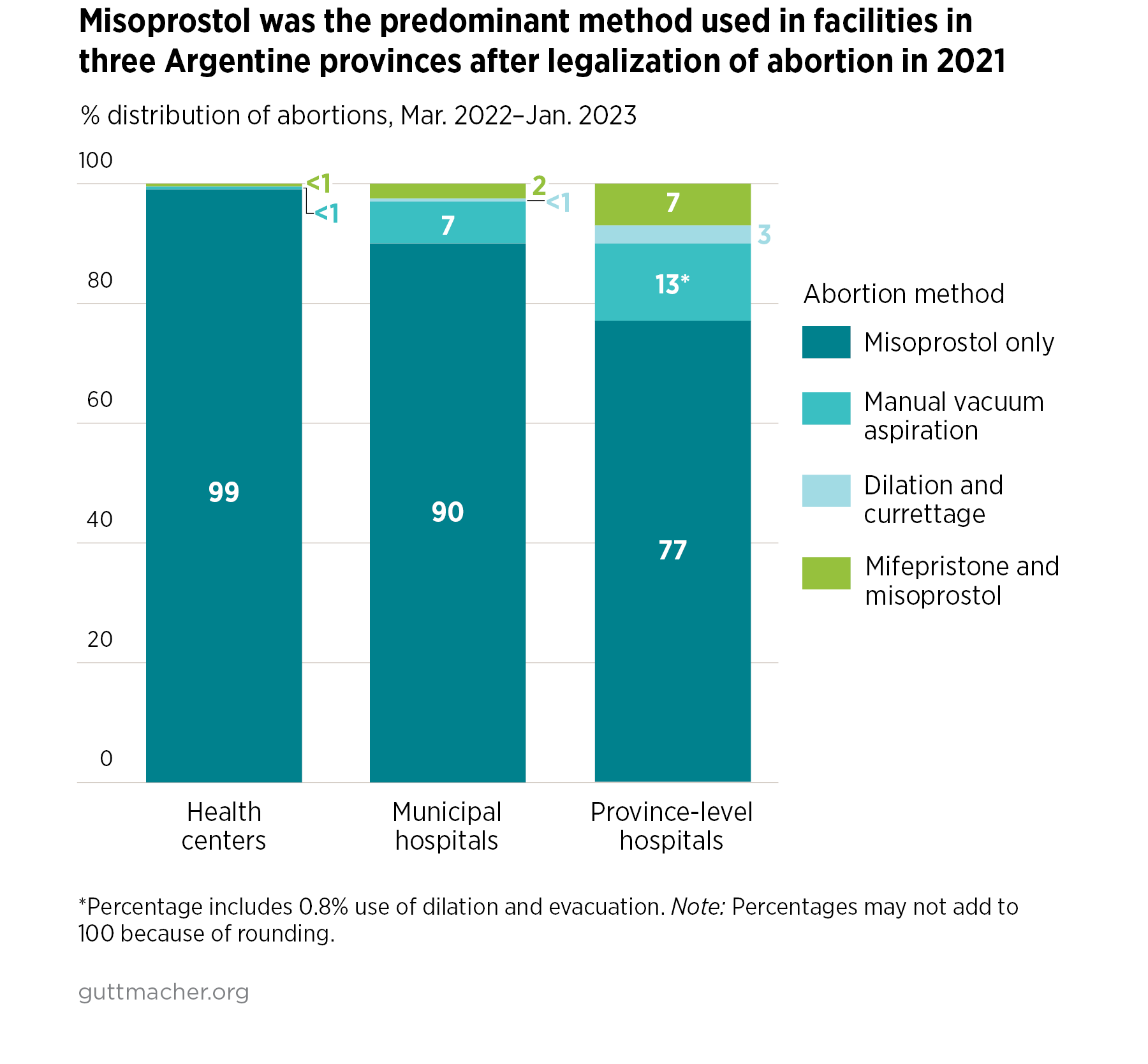
- Among facilities offering abortions, the provision of misoprostol alone accounted for the vast majority of abortions in the facilities surveyed (from 90% in municipal hospitals to 99% in health centers). The lowest proportion, 77%, was in province-level hospitals, which correspondingly performed the highest proportion of surgical abortions.
- Use of the invasive, nonrecommended method of dilation and curettage (D&C) was almost nonexistent.
- Although 100% of all sampled facilities had received training in the use of misoprostol alone, far fewer had staff trained in the medication abortion regimen that combines mifepristone and misoprostol and in the recommended surgical method for later abortions, dilation and evacuation. Indeed, 14–19% of facilities requested more training in the use of the combination protocol and manual vacuum aspiration (mainly health centers), and later abortion techniques (mainly municipal hospitals).
Reasons for not providing abortions
- Among facilities not providing abortions, the second most frequently cited reason was a lack of trained doctors. In province-level hospitals, this was the most frequently cited reason (59%).
- Many facilities had an insufficient number of physicians overall to meet abortion demand. By area, the proportions reporting this issue ranged from 38% in GBA to 18% in the rest of Buenos Aires province. By facility type, 32% of province-level hospitals, 31% of health centers and 15% of municipal hospitals reported they had insufficient personnel.
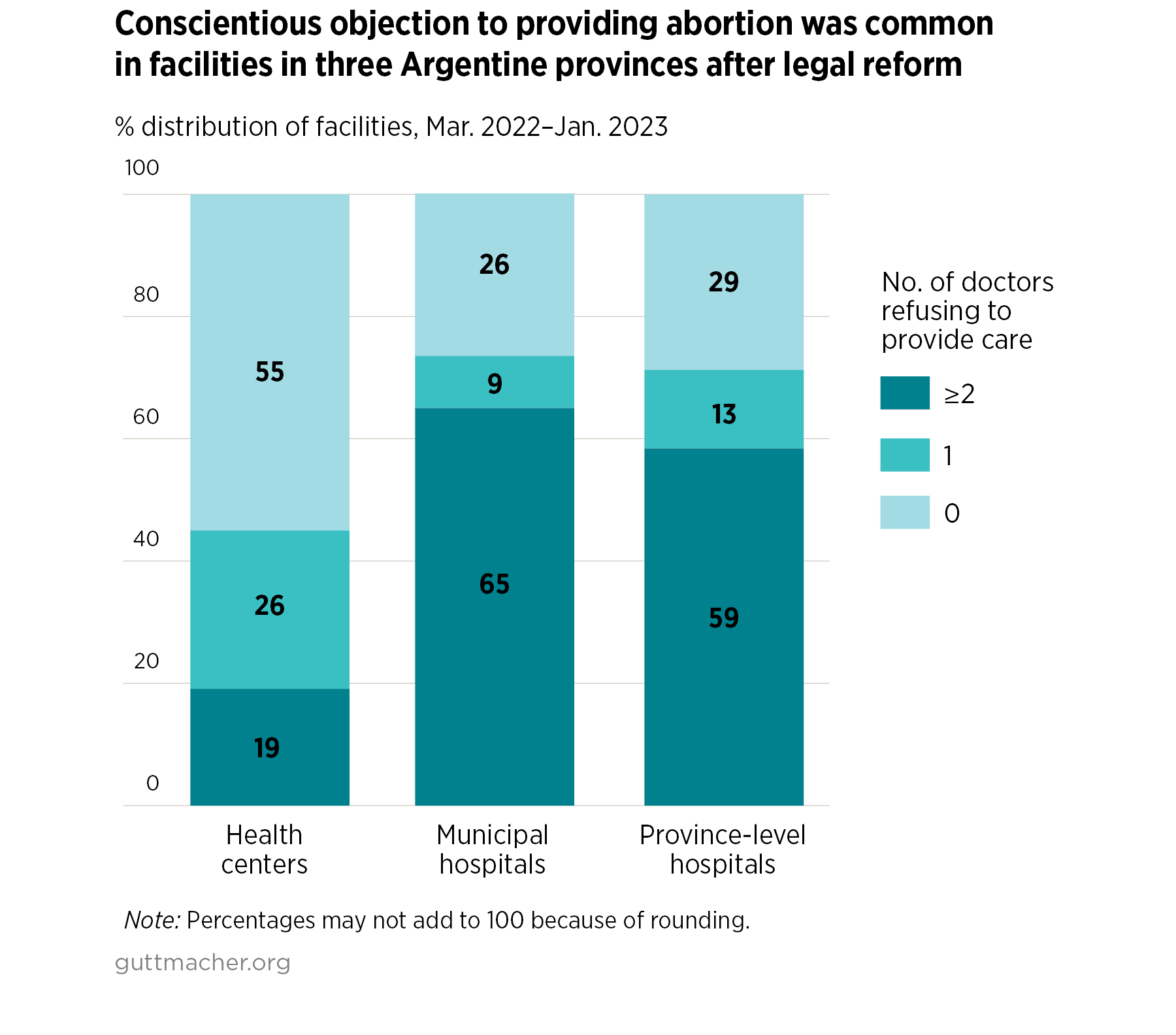
- In facilities that provide abortions, physicians often refused to perform abortions, citing conscientious objection: At least two physicians opted out in 65% of municipal hospitals and 59% of tertiary hospitals. By area, the proportion of facilities with at least two physicians refusing to perform abortions for this reason was highest in La Rioja (57%). In addition, 32% of facilities not providing abortions in La Rioja and 30% of facilities not doing so in the rest of Buenos Aires province (excluding GBA) cited a lack of willing doctors for why abortions were unavailable over the study period.
Conclusion and recommendations
Argentina, the third most populous South American nation, has been at the forefront of the Green Wave, a social and political movement to make abortion safe and legal that is still pushing for change throughout the region.
Official records confirm the law’s immediate positive impact on women’s health: In 2022, no deaths occurred from an unsafely induced abortion in Buenos Aires province.4 It is notable that this was achieved by use of misoprostol in the vast majority of cases in the three provinces surveyed. Although use of the medication abortion regimen combining mifepristone and misoprostol will likely increase now that mifepristone has been approved for sale, our study shows that misoprostol alone can be safely and effectively used for abortion services at scale in public facilities. The minimal use of D&C is also encouraging and is likely the result of decades spent by WHO and international ob-gyn organizations promoting safer surgical techniques—in particular, vacuum aspiration—to replace it.
To further improve abortion access in Argentina, we offer the following recommendations:
- Undertake public information campaigns to emphasize that abortion is legal without restriction as to reason through 14 weeks’ gestation and after that time in several circumstances. Stress in those campaigns the importance of using contraceptives to prevent unintended pregnancy and thus reduce the demand for abortion.
- To overcome reluctance to seek out legal services, widely disseminate the law’s guarantee that patients will be treated with dignity and confidentiality.
- Ensure accurate recordkeeping to track the incidence of safe, legal abortion throughout the public sector.
- Provide training in the combined regimen because fewer facilities had trained staff in the combination regimen than in misoprostol alone.
- Step up training in the recommended methods for later abortions to increase the number of facilities providing abortions after 14 weeks.
- Educate providers about the legal limits to their right to opt out of providing abortion services based on conscientious objection. Medical personnel must be informed that they cannot refuse to perform abortions needed to save a pregnant person’s life or protect their health.
- Implement a system to immediately refer patients to willing and available providers in cases of physicians objecting to provide abortions.
- Train nonmedical personnel on their role in delivering compassionate and nonjudgmental abortion services, a crucial aspect of care that is guaranteed by law.
