Although the 2012 state legislative season is rapidly drawing to a close, some states continue to wrestle with their budgets for the fiscal year that began, in most cases, on July 1. Only seven state legislatures remain in session, and additional states are likely to adjourn in the coming weeks.
In the first half of the year, states enacted 95 new provisions related to reproductive health and rights; issues related to abortion, family planning funding and sex education were significant flashpoints in many legislatures.
For a full accounting of proposals and enactments on a range of reproductive health and rights issues, click here.
Abortion
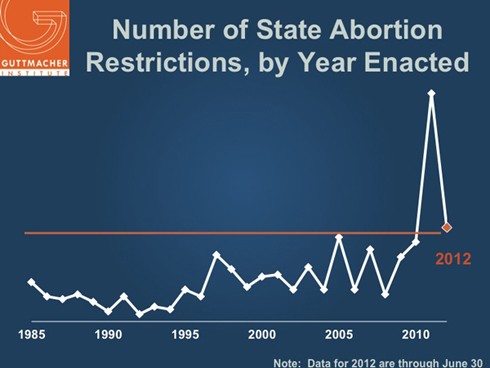
So far this year, states have enacted 39 new restrictions on access to abortion. Although this is significantly lower than the record-breaking 80 restrictions that had been enacted by this point in 2011, it is nonetheless a higher number of restrictions than in any year prior to 2011. Most of the 39 new restrictions have been enacted in one of the states generally hostile to abortion. For example, 14 of the new restrictions have been enacted in just three states—Arizona, Louisiana and South Dakota—that had at least five such restrictions on the books. Fully 55% of women of reproductive age in the United States live in one of the 26 states considered hostile to abortion (see Troubling Trend: More States Hostile to Abortion Rights as Middle Ground Shrinks).
2012 is shaping up to be similar to last year in terms of the number of abortion restrictions that have either been introduced or approved by a legislative chamber. What distinguishes 2012 from 2011, however, is that a lower proportion of the restrictions that were passed by one legislative body have become law—30% of the abortion restrictions passed by one chamber so far this year have been enacted, a significantly lower percentage than the 51% that had been signed into law by this point in 2011.
There are several reasons for this trend. Election-year sessions tend to be shorter, and focus more on bread-and-butter issues, as opposed to social issues. In addition, mirroring the situation nationally, legislatures in states such as New Hampshire and Indiana appear to be in near-total gridlock, seeming able to tackle only “essential” issues relating to spending and basic state services.
At the same time, it appears that public pushback has been successful in blocking action on some of the more extreme abortion restrictions, and that vocal opposition in some states is impeding action on restrictions in others. For example, the outcry against a measure that would have required a woman to undergo a transvaginal ultrasound prior to an abortion in Virginia is widely seen as having blunted the momentum behind similar provisions in Alabama, Idaho and Pennsylvania. Similarly, last November’s defeat of a constitutional amendment in Mississippi that would have conferred personhood at fertilization appears to have helped derail similar provisions in Ohio and Oklahoma in 2012.
Nonetheless, as mentioned above, states have enacted 39 new abortion restrictions so far this year. Three states have limited access to medication abortion, bringing to eight the number of states restricting access to the procedure (see Medication Abortion). Three states have enacted unconstitutional measures that ban abortion prior to fetal viability, either at 18 or 20 weeks postfertilization (which is the equivalent of 20 or 22 weeks after the woman’s last menstrual period); bringing to nine the number of states that have barred abortion after this point (see State Policies on Later Abortion). In addition, four states have moved to limit coverage of abortion in the health exchanges that will be established as part of the implementation of the Affordable Care Act, bringing to 20 the number of states limiting abortion coverage in the exchanges (see Restricting Insurance Coverage of Abortion).
Over the past six months, states appear to have paid particular attention to requiring extended delays for women seeking an abortion. In April, Utah became the first state to require that a woman seeking an abortion wait 72 hours between obtaining counseling and having the procedure; a similar measure was enacted in South Dakota in 2011, but was never implemented because of a legal challenge. Twenty-five other states have a waiting period; these laws generally require that the woman wait 24 hours (see Counseling and Waiting Periods for Abortion).
Also this year, two states adopted measures attempting to use the fetal heartbeat as a way to discourage a woman from seeking an abortion. A new law in Oklahoma requires providers to offer a woman the opportunity to hear the fetal heartbeat when an abortion is performed at or after eight weeks postfertilization (or 10 weeks after the woman’s last menstrual period). A new law in Louisiana requires providers to make the heartbeat audible when a woman is seeking an abortion; this requirement necessitates performing a transvaginal ultrasound for abortions performed in the first eight weeks after the woman’s last menstrual period.
Finally, Arizona and South Dakota adopted measures requiring counseling on the negative mental health consequences of abortion, even though this connection has been widely discredited by mental health experts (see Study Purporting to Show Link Between Abortion and Mental Health Outcomes Decisively Debunked); this brings to nine the number of states requiring counseling to include unsubstantiated information on the mental health impact of having an abortion (see Counseling and Waiting Periods for Abortion). Arizona also enacted a provision that would require a woman seeking an abortion because of a fatal fetal impairment to be given information on the availability of fetal hospice services to provide assistance in carrying the pregnancy to term; Minnesota is the only other state with such a requirement.
Family Planning Funding
Fourteen of the 19 states that include a line-item for family planning have adopted their state budgets as of July. Despite the continuing sad state of state budgets and the widespread attacks on family planning funding last year, no state has singled out family planning funding for draconian cuts so far this year. Ten states maintained level funding for their family planning programs. New Jersey Gov. Chris Christie vetoed a measure that would have restored funding to the state’s program, which was eliminated in 2010. Maine slashed family planning funding by 25%, a cut in line with those taken to other health programs. And surprisingly enough, two states moved to increase funding: Minnesota restored $1 million in funding through the Temporary Assistance to Needy Families (TANF) program, and Virginia increased the 2010 funding level by 23%.
States also seem to be backing away from efforts to defund family planning providers. In 2011, eight states moved to disqualify at least some family planning providers from receipt of state family planning funds; so far this year, only three states have done so. Arizona adopted a measure disqualifying agencies that either provide abortions or that specialize in the provision of family planning services. Kansas and North Carolina disqualified specialized family planning providers from being eligible for state funding; litigation filed shortly after the Kansas provision was adopted has blocked enforcement of the provision, which is identical to one adopted—and enjoined—last year. Aside from the ongoing saga in Texas (see below), no other state has specifically taken aim at Planned Parenthood affiliates by name so far this year.
Moreover, five states have moved to expand eligibility for family planning services under Medicaid. Indiana and Montana became the newest states to adopt a broad expansion, bringing the number of states with income-based expansions to 26 (see Medicaid Family Planning Expansions). The Indiana legislature adopted a measure calling on the state to seek federal approval for the program, which was granted in June; Montana’s application for federal approval, which has been pending for several years, was finally approved in June. Oregon and Washington, which have long-standing Medicaid family planning expansions, increased the income ceilings under their programs from 200% of the federal poverty line to 250%. And finally, the Vermont legislature adopted a measure in March calling on the state to apply for federal approval for an expansion.
Texas’s attempt to link the issues of disqualifying family planning providers and expanding Medicaid family planning expansions stands in sharp contrast to the encouraging developments in other states. A 2011 state law would have prohibited Planned Parenthood affiliates from participating in the state’s long-standing Medicaid family planning expansion. In March, the Centers for Medicare and Medicaid Services informed the state that doing so would violate federal Medicaid requirements. In response, Texas announced that it would instead terminate the federal-state program and establish a state-only effort, in which it would not allow Planned Parenthood affiliates to be reimbursed for the care they provide. At midyear, the future of publicly funded family planning services in Texas remains in flux—litigation filed by Planned Parenthood is pending and the state is moving ahead with plans to establish its new program.
Sex Education
From 2007 through 2010, all the legislation enacted by states related to sex education was aimed at expanding access to comprehensive and medically accurate programs; four states took action during this period. That trend began to reverse in 2011, when Mississippi and South Dakota adopted measures changing their policies to promote abstinence-until-marriage education (see Sex and HIV Education).
So far this year, Wisconsin and Tennessee have joined the fray by adopting measures promoting abstinence-until-marriage education. In April, Wisconsin rolled back its 2010 law mandating comprehensive sex education and substituted a measure requiring information about the benefits of abstinence until marriage; the 2012 law does not even identify discussion of contraception as a recommended topic. For its part, Tennessee amended its law to require that any sex education in the state “exclusively and emphatically” teach abstinence and provide instruction on the consequences of “nonmarital” sex. Contraception education may be included only if it does not promote sex among unmarried students and informs students that contraception does not eliminate the risk of pregnancy and STIs. Also in 2012, Utah Gov. Gary Herbert vetoed a measure that would have prohibited any discussion of contraception or homosexuality in sex education in the state—but only because it was included in a larger bill that would have rolled back a requirement that abstinence education be taught in all school districts.