Investments in sexual and reproductive health and rights (SRHR) are among the most cost-effective development interventions available. Supporting SRHR improves health, prevents unintended pregnancies, reduces maternal and infant mortality, and expands educational and economic opportunities for women and girls. The evidence is clear: Funding for sexual and reproductive health is central to resilient health systems, human rights, gender equality and sustainable development.
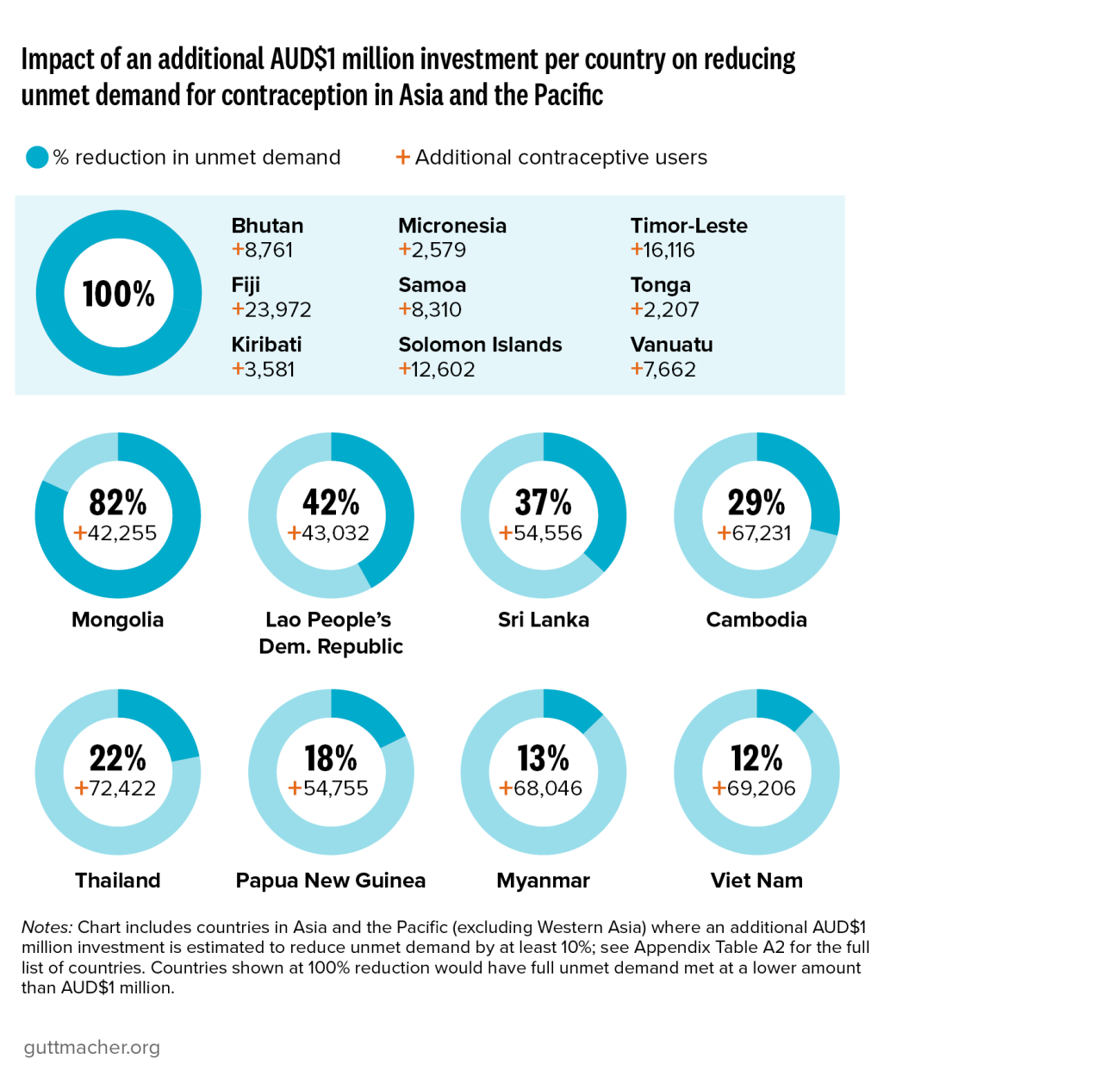
In Asia and the Pacific,* the need for comprehensive sexual and reproductive health services remains substantial, driven by persistent gaps in health system capacity, geographic barriers to service delivery, and increasing vulnerability to humanitarian crises and climate-related disasters. These challenges contribute to significant gaps in access to essential services, including contraception, safe abortion care, and maternal and newborn health services.
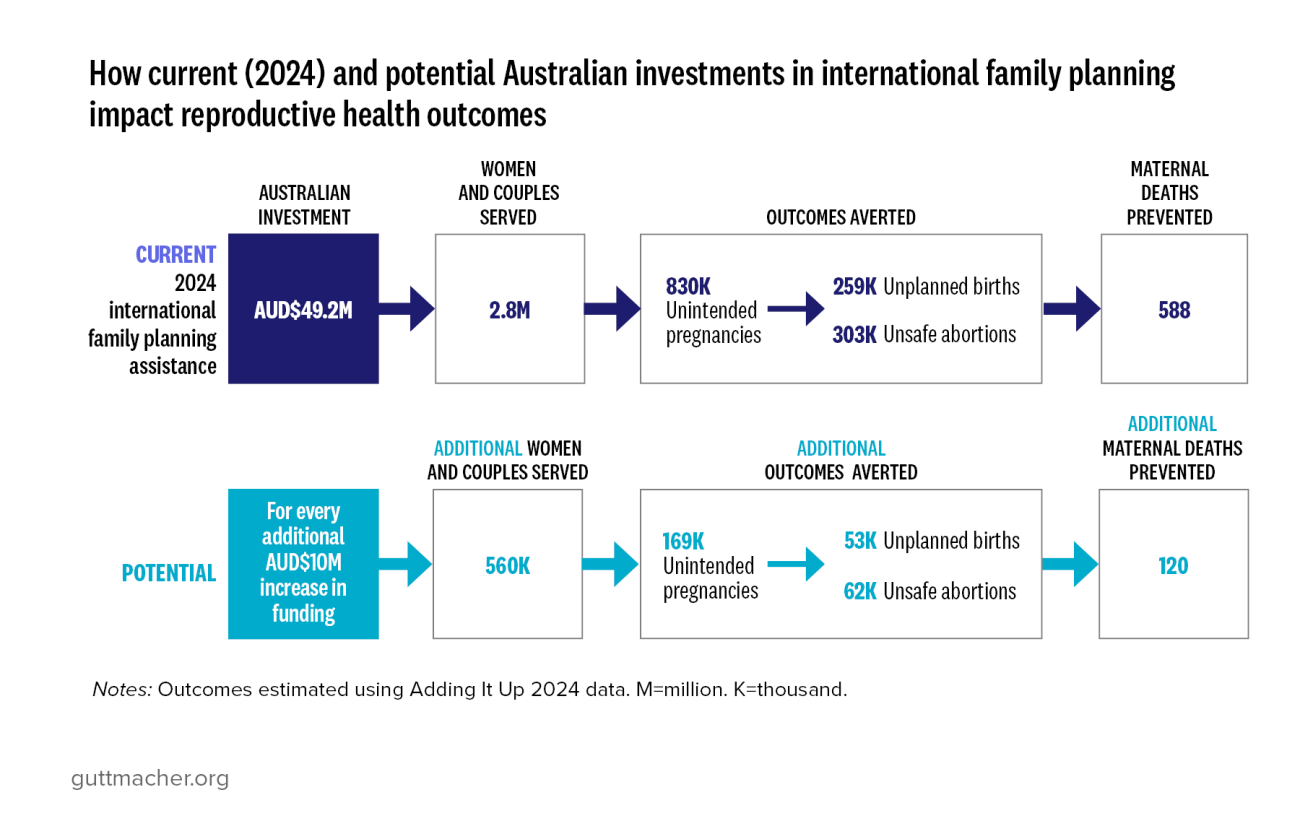
As one of the region’s most established development partners, Australia is uniquely positioned to contribute in response to these needs, ensuring that services that support and expand SRHR reach the populations most in need. The country has a long-standing commitment to health, gender equality and support for resilient, inclusive health systems and communities across the region, with a particular emphasis on the Southeast Asia subregion and the Pacific region. In 2023, approximately 2.8% of Australia’s official development assistance was directed toward SRHR, and Australia ranked 12th among donor countries by the share of such assistance dedicated to SRHR.1