- Malawi’s maternal mortality ratio remains one of the highest in the world—574 maternal deaths per 100,000 live births in 2014—and maternal deaths present a major public health challenge for the country.1
- The majority of induced abortion procedures in Malawi are performed under clandestine and unsafe conditions. Complications from abortions have been estimated to account for between 6% and 18% of maternal deaths in Malawi.2,3
- Abortion is only legal in Malawi to save a woman’s life. Obtaining an abortion for any other reason is punishable by 7–14 years in prison.4
- A national debate is currently under way on whether or not to liberalize Malawi’s abortion law by providing more exceptions under which an abortion could be legally obtained.5
Incidence of induced abortion
- In Malawi, an estimated 141,000 abortions were performed in 2015. This number translates to a rate of 38 abortions per 1,000 women aged 15–49.
- Within Malawi, abortion rates vary widely by region, from 29 per 1,000 women in the Central region to 61 in the Northern region.
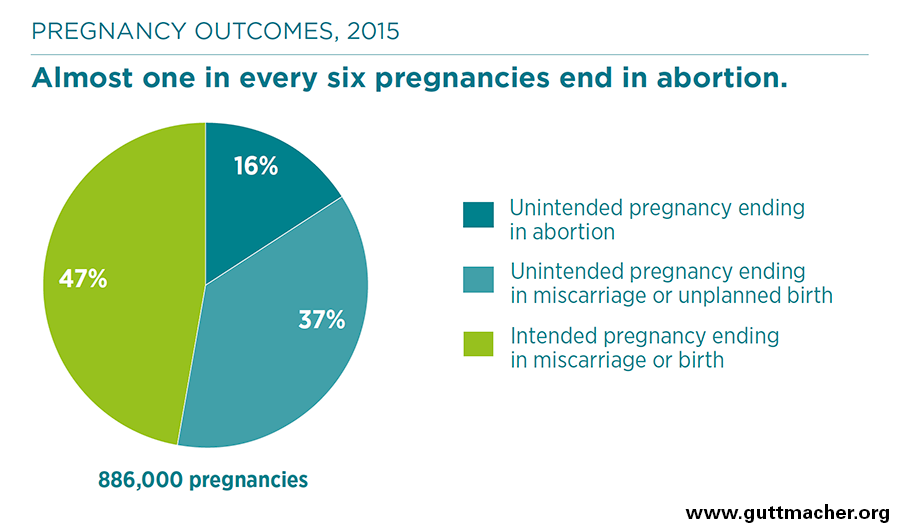
- In Malawi in 2015, 39% of pregnancies ended in planned births, 30% in unplanned births, 16% in abortion and 15% in miscarriages.
- Malawi’s abortion rate is similar to other countries in the region, including Tanzania (36 per 1,000 women) and Uganda (39), as well as to the regional rates for Eastern Africa (34) and Southern Africa (35).6,7,8
- A 2009 study estimated a substantially lower abortion rate in Malawi than the new estimated rate for 2015.9 Due to several methodological differences between the two studies, it is not possible to infer a trend on the basis of these two studies.
Availability of postabortion care
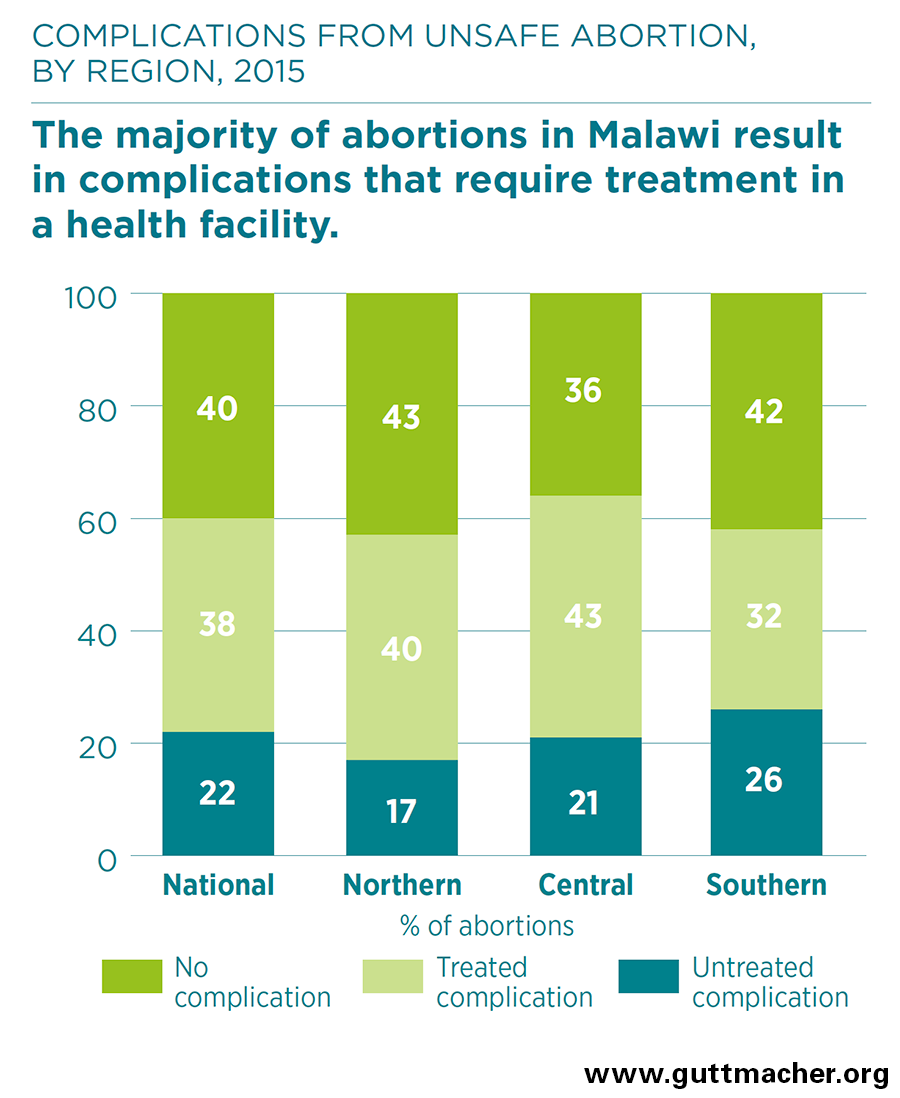
- Out of the estimated 141,000 abortions performed in Malawi in 2015, approximately 60% resulted in complications that required medical treatment in a health facility.
- An estimated one-third of the women who experienced complications from an abortion did not receive the medical treatment they needed.
- The annual treatment rate for complications from abortion was estimated to be 14 per 1,000 women aged 15–49 in 2015.
- A 2009 study estimated that more than one in four women who reached a health care facility for postabortion care had severe or moderate complications.10
- The majority of Malawi’s postabortion care cases are treated at district hospitals (35%), health centers (22%) and clinics (20%).
- Treating complications of unsafe abortion represents a significant financial burden for the national health system in Malawi. A 2009 study estimated that a liberalized abortion law and access to safe abortion in public health facilities would yield a 20–30% decrease in postabortion care costs for the health system.11
Impact of unintended pregnancy
- Globally, most abortions are the result of unintended pregnancy. In Malawi, 53% of pregnancies in 2015 were unintended, and close to one-third (30%) of these unintended pregnancies ended in abortion.
- Modern contraceptive use has increased substantially over the past decade in Malawi. Among married women aged 15–49, modern contraceptive use increased from 28% in 2004 to 58% in 2015. Among sexually active unmarried women in this age-group, usage increased from 24% in 2004 to 43% in 2015. Use of traditional contraceptive methods—which can have high failure rates—is extremely low in Malawi.12,13
- Meeting women’s contraceptive needs is a critical step toward decreasing the incidence of unintended pregnancies, as well as the unsafe abortions and maternal deaths and injuries that often result from these pregnancies.
- In Malawi, one in five married women and two in five sexually active unmarried women of reproductive age have an unmet need for contraception.13 That is, they want to avoid a pregnancy but are not using any contraceptive method.
Recommendations
- Ensure that free or affordable family planning services reach all individuals to reduce unmet need for contraception and lower the incidence of unintended pregnancy. Programs should offer comprehensive family planning services—including counseling for and availability of a wide range of contraceptive methods—to enable women and couples to choose the methods that work best for them, to use methods effectively and to switch methods when desired. These programs should make special efforts to reach rural and poor Malawian women, who experience higher levels of unmet need for family planning than their urban and nonpoor counterparts.
- Expand postabortion care services by guaranteeing that all health facilities are fully stocked with the necessary medications, supplies and equipment to provide this care, and that staff are trained in how to provide postabortion care according to World Health Organization guidelines.
- Ensure that policy discussions in Malawi on abortion consider the full range of available evidence around reducing maternal mortality and morbidity, and acknowledge that expanding access to safe abortion care would reduce the number of women who experience complications from unsafe abortion.