• Tanzania has one of the highest maternal mortality ratios in the world (410 per 100,000 live births), and unsafe abortion is one of its leading causes.
• Unsafe abortions account for more than one-third of hospitalizations for complications related to pregnancy1 and roughly one-quarter of maternal deaths.2,3
• Laws and policies on abortion in Tanzania are ambiguous and often confusing. The Penal Code is broadly understood to authorize abortion to save a woman’s life, but is unclear about whether the procedure is legal to preserve the woman’s physical or mental health.4 The fear of prosecution, prevalent among women and health care providers alike, drives women to seek clandestine abortions that are often unsafe.
ABORTION INCIDENCE
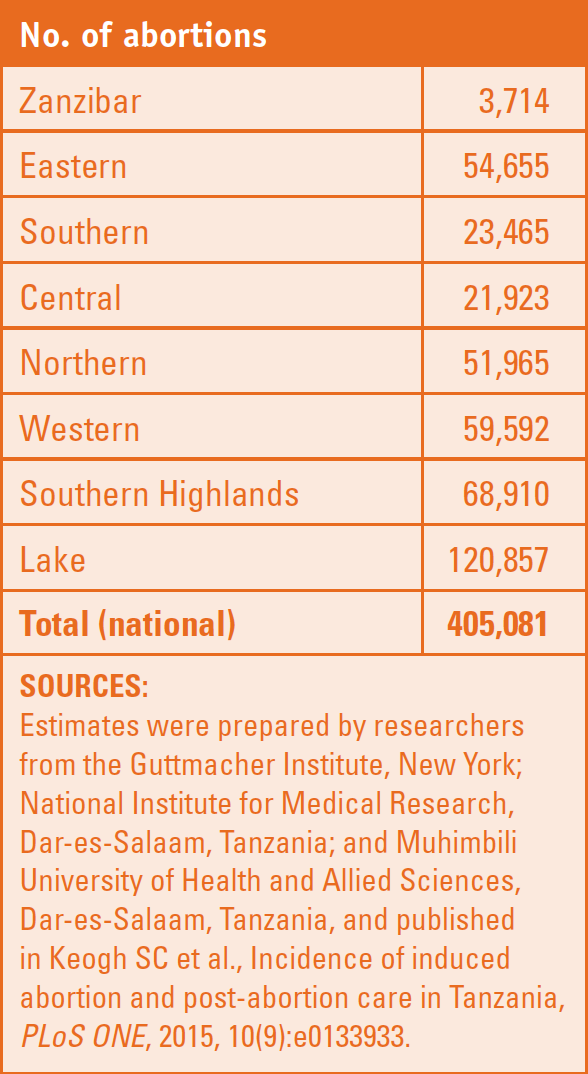
• In Tanzania, an estimated 405,000 abortions were performed in 2013. This number translates to a rate of 36 abortions per 1,000 women aged 15–49 and a ratio of 21 abortions per 100 live births.
• The abortion rate is the same as the estimated rate for the East Africa region as a whole (36 per 1,000 women) and slightly higher than the rate for Sub-Saharan Africa (31).5
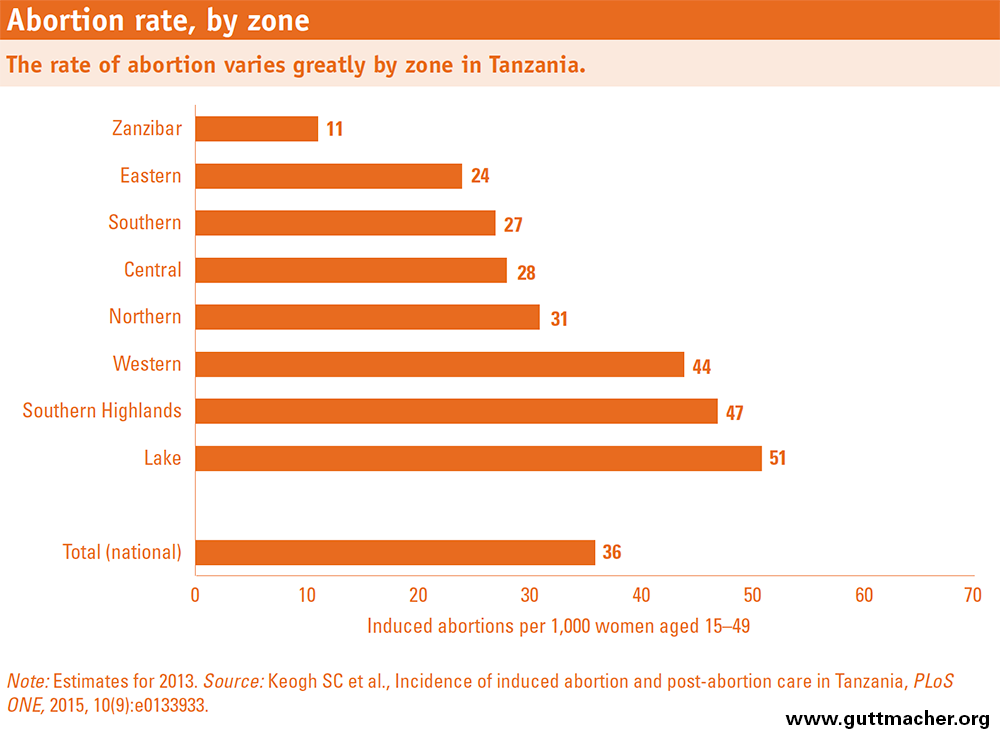
• Within Tanzania, abortion rates vary widely by zone, from 11 per 1,000 women in Zanzibar to 47 in the Southern Highlands and 51 in the Lake zone. The Lake zone and Southern Highlands also have high rates of treatment for complications of induced abortion.
• In 2013, in the country as a whole, 15% of pregnancies ended in abortions, 52% in intended births, 18% in unintended births and 15% in miscarriages. These distributions vary across zones—for example, the proportion of pregnancies ending in abortion ranges from 6% in Zanzibar to 18% in the Southern Highlands.
FACTORS UNDERLYING ABORTION RATES
• Several factors explain the variation in abortion rates by zone: differences in the number of children that women wish to have, in levels of sexual activity and contraceptive use, and in women’s likelihood of resorting to abortion in the event of an unintended pregnancy.
• About one in five women aged 15–49 in Tanzania wants to delay or stop having children but is not using any contraceptive method. This group of women is considered to have an unmet need for family planning.
• In the Lake zone, low contraceptive use (the lowest in the country) and high unmet need contribute to the zone’s high abortion rate and unintended pregnancy rate, which is the highest in the country.
• In the Southern Highlands, where contraceptive use is high, women with unintended pregnancies are more likely to resort to abortion than those in other zones, resulting in higher abortion rates: 59% of unintended pregnancies ended in abortion in the Southern Highlands in 2013, compared with less than 45% in other zones.
• Zanzibar’s relatively low abortion rate, at 11 per 1,000 women aged 15–49, is mainly due to its having the lowest unintended pregnancy rate in the country. Compared with their Mainland counterparts, women in Zanzibar tend to initiate sexual activity at a later age, and married women report lower levels of sexual activity.
AVAILABILITY OF POSTABORTION CARE
• In Tanzania in 2013, nearly 67,000 women were treated in health facilities for complications resulting from unsafe abortions. However, almost 100,000 other women who experienced complications requiring treatment in a health facility did not receive the medical attention they needed.
• Referral and regional hospitals treat the majority of Tanzania’s postabortion care cases; on average, they each treated about 1,140 and 710 cases in 2013, respectively.
• On average, just under eight facilities provide postabortion care for every 100,000 women in Tanzania. Zanzibar is the best served, with more than 10 facilities per 100,000 women, while the Eastern zone has the fewest services—fewer than six per 100,000.
• Treatment rates for abortion complications differ widely by region, partly because of the unequal distribution of post–abortion care providers.
STRENGTHENING POSTABORTION CARE AND CONTRACEPTIVE SERVICES
• Reducing unsafe abortions and the maternal deaths and injuries associated with them will require expanding access to contraceptive services (to prevent unintended pregnancies) and to postabortion care.
• Facilities at all levels should be fully stocked with the necessary drugs, supplies and equipment to provide basic postabortion care, and midlevel providers should be trained to provide such care.
• Postabortion care should work in tandem with contraceptive services because postabortion patients are highly receptive to contraceptive counseling.6,7 Studies have found that the vast majority of these patients adopt a contraceptive method and continue using it.8
• Postabortion care also provides an opportunity to involve men in family planning: Men accompanying their partners for postabortion care have been found to be receptive to contraceptive information.9
• Placing priority on the zones with the highest abortion rates, such as the Lake zone and the Southern Highlands, would be a cost-effective way to reduce maternal mortality and morbidity in Tanzania.
• Ambiguity about the abortion law in Tanzania should be clarified to support safe and legal procedures to the full extent allowed, and to ensure that women do not needlessly resort to unsafe procedures to terminate their pregnancies.