
Updated on December 1, 2022:
This analysis, originally published in June 2022, shared pre released data from Guttmacher’s census of all known abortion providers. The full paper with additional findings was published on November 20, 2022, and is available here.
First published on June 15, 2022:
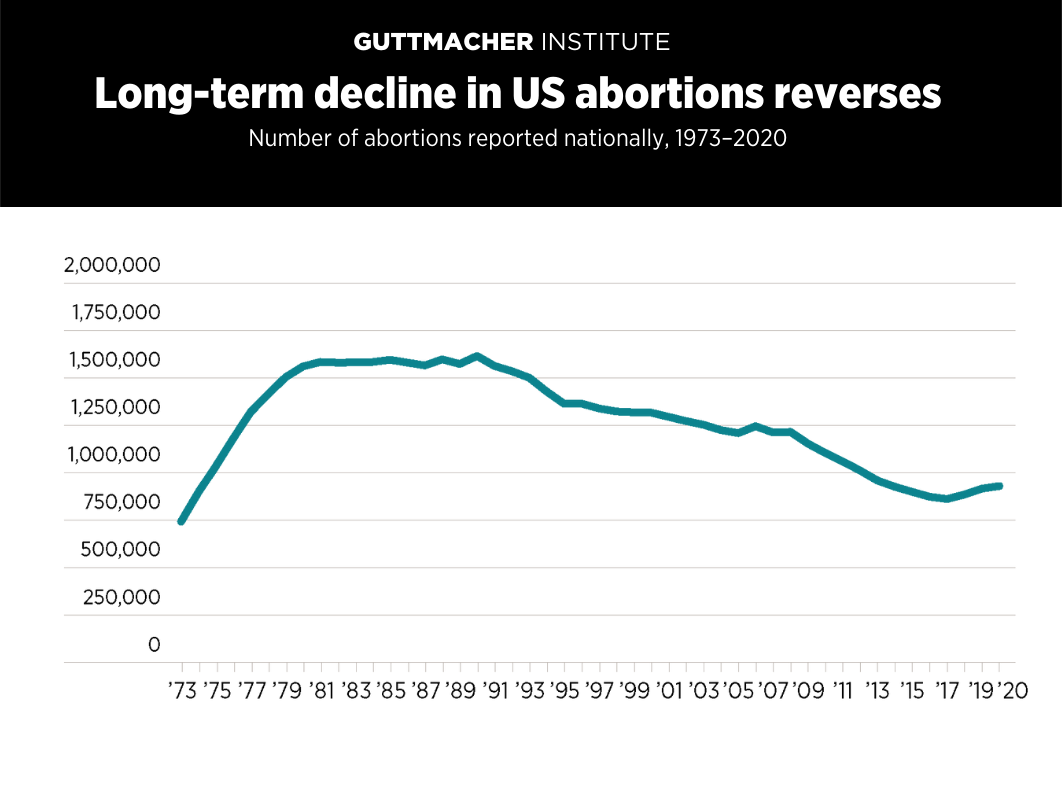
The long-term decline in abortions in the United States that started 30 years ago has reversed, according to new data from the Guttmacher Institute—underscoring that the need for abortion care in the United States is growing just as the US Supreme Court appears likely to overturn or gut Roe v. Wade.
According to new findings from Guttmacher’s latest Abortion Provider Census—the most comprehensive data collection effort on abortion provision in the United States—there were 8% more abortions in 2020 than in 2017.
A recently leaked draft of the Supreme Court majority opinion in Dobbs v. Jackson Women’s Health Organization would explicitly overturn Roe and 50 years of the Court’s own legal precedent upholding the constitutional right to abortion. States have been ramping up their attacks on abortion rights and access in anticipation of the Court’s decision, and 26 states are certain or likely to quickly ban abortion without Roe. People with very few resources and those who are already marginalized bear the brunt of abortion bans and other restrictive policies.
An increase in abortion numbers is a positive development if it means people are getting the health care they want and need. Rather than focusing on reducing abortion, policies should instead center the needs of people and protect their right to bodily autonomy.
Overall Increase in Abortion Nationwide
The new data released by Guttmacher include several notable trends (see table with abortion incidence and rates by state and region):
- In 2020, there were 930,160 abortions in the United States, an 8% increase from 862,320 abortions in 2017.
- Similarly, the abortion rate increased from 13.5 abortions per 1,000 women aged 15–44 in 2017 to 14.4 per 1,000 women, a 7% increase.
- In 2020, about one in five pregnancies ended in abortion. More specifically, the abortion ratio (the number of abortions per 100 pregnancies) increased from 18.4% in 2017 to 20.6% in 2020, a 12% increase.
- The increase in abortion was accompanied by a 6% decline in births between 2017 and 2020. Because there were many more births (3.6 million) than abortions (930,000) in 2020, these patterns mean that fewer people were getting pregnant and, among those who did, a larger proportion chose to have an abortion.
- The number of abortions increased in all four regions of the country between 2017 and 2020. The rise was largest in the West (12% increase) and Midwest (10% increase); abortions increased 8% in the South and 2% in the Northeast.
Interpreting the Overall Increase in Abortion
While abortion increased nationally, there was substantial variation across, and even within, states between 2017 and 2020. A number of developments over that period may have had differential impacts across states.
- Some states expanded Medicaid coverage of abortion care. The majority of people who obtain an abortion are poor or low income, and this coverage meant that many who would not otherwise have been able to afford an abortion could get care.
- The Trump-Pence administration’s "domestic gag rule" dramatically slashed the Title X family planning network’s capacity and severely reduced the number of contraceptive clients served by the program. This meant that many people in some states lost access to low- or no-cost contraceptive care. In turn, this may have resulted in more unintended pregnancies and greater need for abortion care.
- Local and national abortion funds increased their capacity and helped even more people pay for their abortions.
- The COVID-19 pandemic disrupted health care systems across the United States. Some states attempted to ban abortion access early in the pandemic, falsely claiming it was not essential health care. Abortion access was also disrupted in some states supportive of abortion rights because health care providers were dealing with outbreaks of COVID-19 among their families and communities. Still other states were able to maintain steady access to abortion care, including for people from states where it was not accessible due to the pandemic.
- Between 2017 and 2020, 25 states enacted 168 abortion restrictions and bans, but not all of them went into effect because of legal challenges. In addition, many of these new restrictions were enacted in states where clinics had already been operating in hostile environments, so their practical effect likely was reduced.
- During this time period, 75 provisions to protect abortion rights were enacted. Half of these measures repealed pre-Roe bans or other restrictions. Among the other half, many expanded access by requiring Medicaid or private health plans to cover abortion, or allowing qualified clinicians such as nurse practitioners, physician assistants or certified nurse midwives to provide at least some abortion care.
- Because restrictions were adopted in states generally considered hostile to abortion rights already, they may not have played as much of a role as the measures expanding access, particularly policies that help people pay for abortion care.
Abortion Trends Varied Across States
Abortion trends varied across states between 2017 and 2020 and there were no clear patterns to explain why some had increases or decreases.
In some states—including Illinois, Mississippi and Oklahoma—there were substantial increases in the number of abortions. In others—such as Missouri, Oregon and South Dakota—there were substantially fewer abortions in 2020 compared with 2017.
Below, we highlight a few states and offer policy context that may have contributed to recent changes in their abortion numbers.
- New York: Abortion incidence increased 5% between 2017 and 2020, but with differing patterns across the three-year period. After substantially increasing between 2017 and 2019, the number of abortions declined 6% between 2019 and 2020. New York was one of the first states to be affected by COVID-19 and among the hardest hit. At least 10% of clinics in the state reported that they paused or stopped providing abortion care in 2020.
- Illinois: Abortion incidence increased 25% between 2017 and 2020, with almost all of the increase (24%) occurring between 2017 and 2019. Some of this was due to more people coming from surrounding states like Missouri, but abortion also increased substantially among Illinois residents. One likely contributing factor is that Illinois allowed the use of state Medicaid funds to pay for abortion care starting in January 2018. Another factor is Illinois had more abortion clinics in 2020 than in 2017 (30 and 25, respectively) and this also may have made abortion more accessible.
- Missouri: The number of abortions decreased from 4,710 in 2017 to 170 in 2020. Even in 2017, the majority of Missouri residents went out of state for abortion care. This pattern was magnified between 2017 and 2020, and the number of Missouri residents who obtained abortions in Illinois, in particular, increased substantially.
- Mississippi: The number of abortions increased 40% between 2017 and 2020. Mississippi has only one abortion clinic and, in the past, facilities in neighboring states were closer for many Mississippi residents. However, as neighboring states became more restrictive and experienced clinic closures, more Mississippi residents obtained abortion care in their state of residence.
- Maine: Abortion incidence increased 16% between 2017 and 2020, with most of the increase taking place between 2019 and 2020. In January 2020, Maine allowed the use of state Medicaid funds to pay for abortion care and required private health insurance plans to cover abortion, and these are likely factors behind the increase.
- Texas: The number of abortions increased 7% between 2017 and 2019, followed by a decrease of 2% between 2019 and 2020. One factor that likely contributed to the drop was the state’s near-total ban on abortion provision as part of broader COVID-19 restrictions imposed by the Texas governor, when he deemed abortion "nonessential" health care at the beginning of the pandemic.
- Florida: The number of abortions increased 9% between 2017 and 2020, with most of the increase (7%) taking place between 2019 and 2020. More people from other states obtained abortions in Florida in 2020 than in the prior year, potentially because they lived in neighboring states that imposed restrictions on abortion care as "nonessential" under COVID-19 orders, such as Alabama.
Implications
The Supreme Court is poised to overturn Roe v. Wade at a time when need for abortion care has been increasing—including in many of the 26 states likely to ban abortion following the Court’s official decision on the Mississippi case. This means the impact of the ruling could be even more devastating than predicted by prior analyses, particularly for people across the country who already struggle to access abortion care.
Methodology
Every three years, the Guttmacher Institute contacts all known facilities providing abortion in the United States to collect information about service provision, including total number of abortions. The most recent Abortion Provider Census was completed in May 2022, and data represent 1,687 health care facilities that provided abortions in 2019 or 2020.
Fifty-two percent of facilities provided responses to our questionnaire or by phone or email when contacted for follow-up. We were able to use state health department data to determine the number of abortions provided at 17% of facilities and the total number was estimated for the remaining 31%. Notably, most of the facilities for which we had to make estimates were hospitals, which typically perform only a small number of abortions annually. In total, 84% of the abortions we counted were based on information provided by health care facilities directly.
Our counts only include provision of abortion overseen by clinicians and do not account for self-managed abortion.
Pregnancies include births and abortions but do not include miscarriages.
See here for a table with abortion incidence and rates by state and region. A fuller summary of the data will be published later this year in a peer-reviewed journal article.
The authors thank the fielding staff for their invaluable data collection efforts that made this report possible: Lilian Ha, Madeleine Haas, Audrey Maynard, Rayan Sadeldin Bashir Mohamed and Parisa Thepmankorn.