This fact sheet summarizes findings for Bihar from a 2015 study that provides the first comprehensive estimates of the incidence of abortion and unintended pregnancy in six states in India.
Incidence of abortion and unintended pregnancy
- Induced abortion has been legal in India on a broad range of grounds since the Medical Termination of Pregnancy (MTP) Act was passed in 1971.*
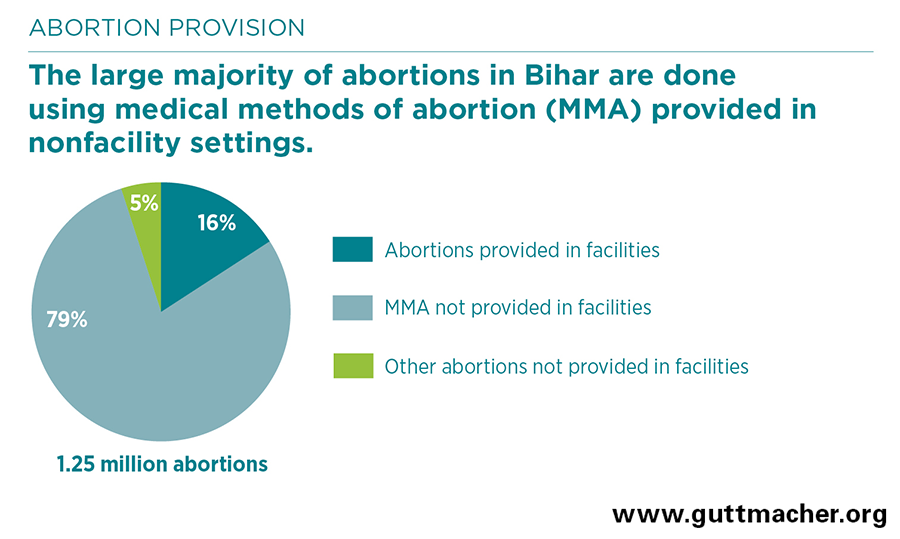
- An estimated 1.25 million abortions are performed in Bihar annually. For 2015, this translates to 49 abortions per 1,000 women of reproductive age (15–49).
- Sixteen percent of abortions occurring annually in the state—an estimated 194,300—are provided in health facilities. About three-quarters of these are surgical and one-quarter are performed using medical methods of abortion (MMA).† Eighty-eight percent of facility-based abortions are provided in private facilities, nearly 8% in public facilities and about 5% in NGO facilities.
- The large majority of abortions in Bihar (79%) are done using MMA obtained in settings other than health facilities. Five percent are performed outside of health facilities using other, typically unsafe methods.
- An estimated 48% of all pregnancies in the state—2.26 million in 2015—are unintended. More than half (55%) of these unintended pregnancies end in abortion.
Postabortion care
- Each year in Bihar, roughly 360,500 women obtain facility-based postabortion care for complications resulting from induced abortion or miscarriage.
- The majority of women receiving post-abortion care are treated for minor complications, such as incomplete abortion from MMA or prolonged or abnormal bleeding, and many of these women likely seek care unnecessarily because they mistake the normal process of MMA for a complication.
- An important minority of postabortion care patients experience one or more severe complication, such as infection (16%), physical injury (9%), sepsis (5%) or shock (4%). These complications are most likely the result of nonfacility abortions using methods other than MMA.
Provision of abortion-related care in health facilities
- As of 2015, an estimated 2,834 facilities in Bihar provide abortion-related care (induced abortion, postabortion care or both types of services); 22% of these facilities are public and 78% are private (including NGOs).
- Among facilities offering any abortion-related care, about 59% provide both induced abortion and postabortion care, 34% offer only postabortion care and 6% offer only abortion.
- Only 30% of public facilities offer any abortion-related care. This includes the majority of higher-level public facilities—77% of hospitals and 59% of community health centres—but only 23% of primary health centres.
- Although 87% of women in Bihar reside in rural areas, just 31% of facilities offering abortion-related services are located in these areas.
Types of abortions provided in facilities
- The vast majority (91%) of facility-based abortions take place in the first trimester of pregnancy (up to 12 weeks’ gestation), and more than half occur in the first seven weeks of pregnancy.
- More than two-thirds of facility-based abortions are performed using the techniques recommended for early termination: manual or electric aspiration (43%) and MMA (27%). Although only 9% of facility-based abortions occur after the first trimester, 31% are performed using more invasive surgical procedures not recommended in the first trimester (dilatation and evacuation or dilatation and curettage).
Barriers to obtaining facility-based abortion
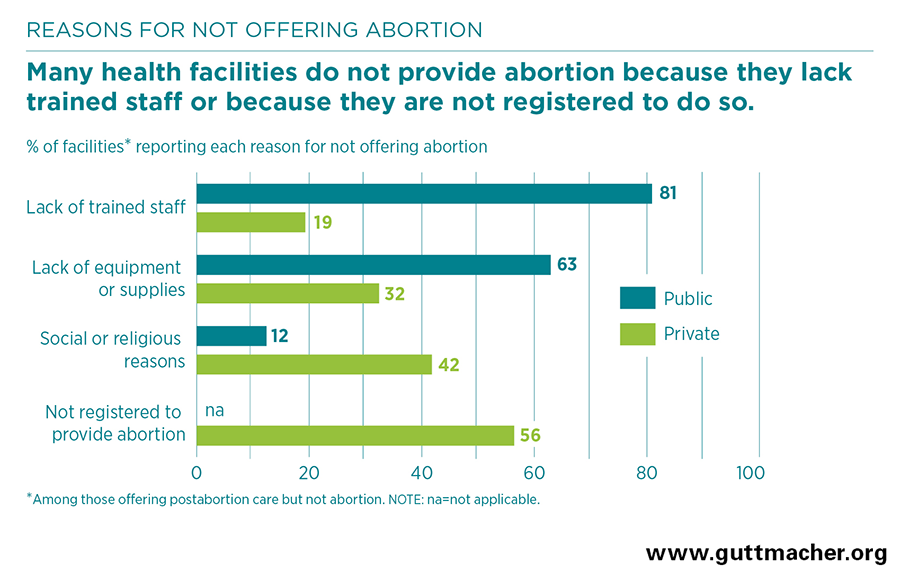
- In Bihar, 64% of public facilities that offer any abortion-related services provide only postabortion care. Among these facilities, the most common reasons reported for not offering induced abortion are lack of trained staff and lack of equipment or supplies.
- Unlike public facilities, which are automatically approved to provide induced abortion if they have a certified provider, private facilities must obtain registration before offering that service. Among private facilities offering any abortion-related care, 26% offer only postabortion care; for them, lack of registration is the most common reason for not providing abortion.
- Staff at health facilities cite fear of social stigma as a key barrier preventing women from obtaining safe abortion care. Other such barriers include cost and a lack of information about services.
- Moreover, some abortion providers deny women services for reasons that are not in keeping with national abortion guidelines, including because the women are perceived to be too young, are unmarried, do not have children or do not have consent from a family member.
Recommendations
- Improve access to facility-based abortion services, especially in underserved rural areas, by ensuring that all public-sector facilities have adequate equipment and supplies, including MMA drugs.
- Expand the number of providers trained in abortion-related services, for example, by offering MMA training for current and new providers and by amending the MTP Act to allow nurses, auxiliary nurse midwives and practitioners trained in Indian systems of medicine to provide MMA and postabortion care.
- Streamline the process for registering private facilities to offer abortion services by ensuring that District Level Committees are functional, and expand the registration process to include those facilities that are providing MMA only.
- Ensure high-quality abortion care that adheres to national guidelines by training providers in current abortion techniques and best practices, in national abortion laws and in nonjudgmental service provision.
- Use community-based health workers and public health campaigns to educate women about the availability of safe, legal abortion services in facilities, and inform them about the correct use of MMA and the abortion process following its use.
- Improve the quality and availability of voluntary contraceptive services for all women, including those receiving abortion and postabortion services, to help them prevent future unintended pregnancies. Services should include provision of a wide range of methods, counseling on consistent and correct use, and facilitation of method switching.