This fact sheet highlights key data points related to abortion in the United States, drawing on the Guttmacher Institute’s long-standing efforts to document abortion numbers and rates, characteristics of people having abortions and related indicators.
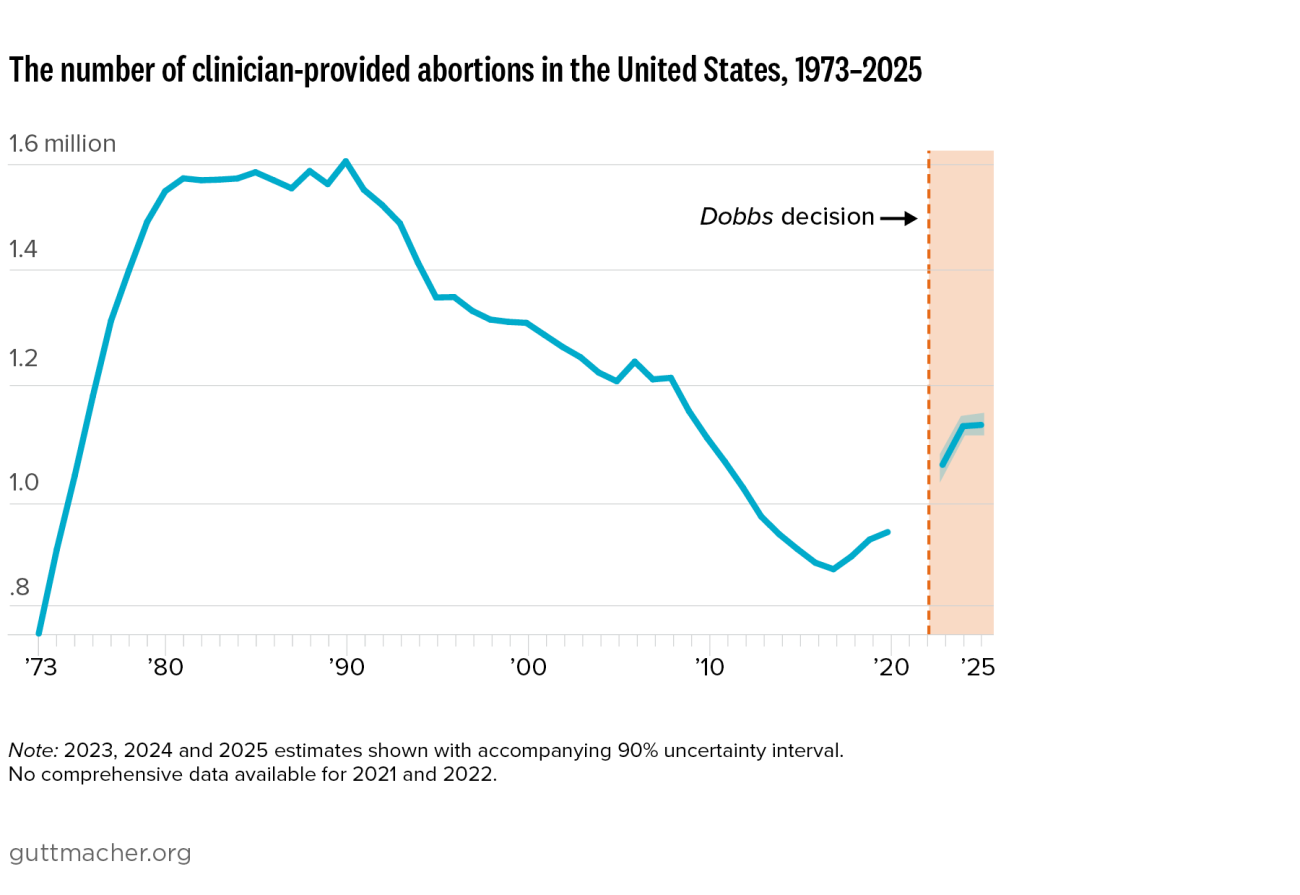
The US abortion policy landscape continues to evolve in the wake of the Supreme Court’s June 2022 decision in Dobbs v. Jackson Women’s Health Organization, which overturned Roe v. Wade. The latest information on abortion policies in effect in each state—including total abortion bans and other restrictions—can be found on Guttmacher’s interactive abortion policy map.
Numbers and Rates
- An estimated 1,126,000 abortions were provided by US clinicians in 2025, largely unchanged from 2024, when there were 1,124,000 clinician-provided abortions, and an increase of 21% from 2020, the last year of comprehensive national estimates before Dobbs.1 This count includes medication abortions provided via telemedicine by US clinicians, including those provided under the protection of shield laws to patients in states with total bans. It does not include self-managed abortions, such as those using medications mailed from pharmacies outside the United States or sourced from community networks. Evidence suggests self-managed abortions have increased since Dobbs.2