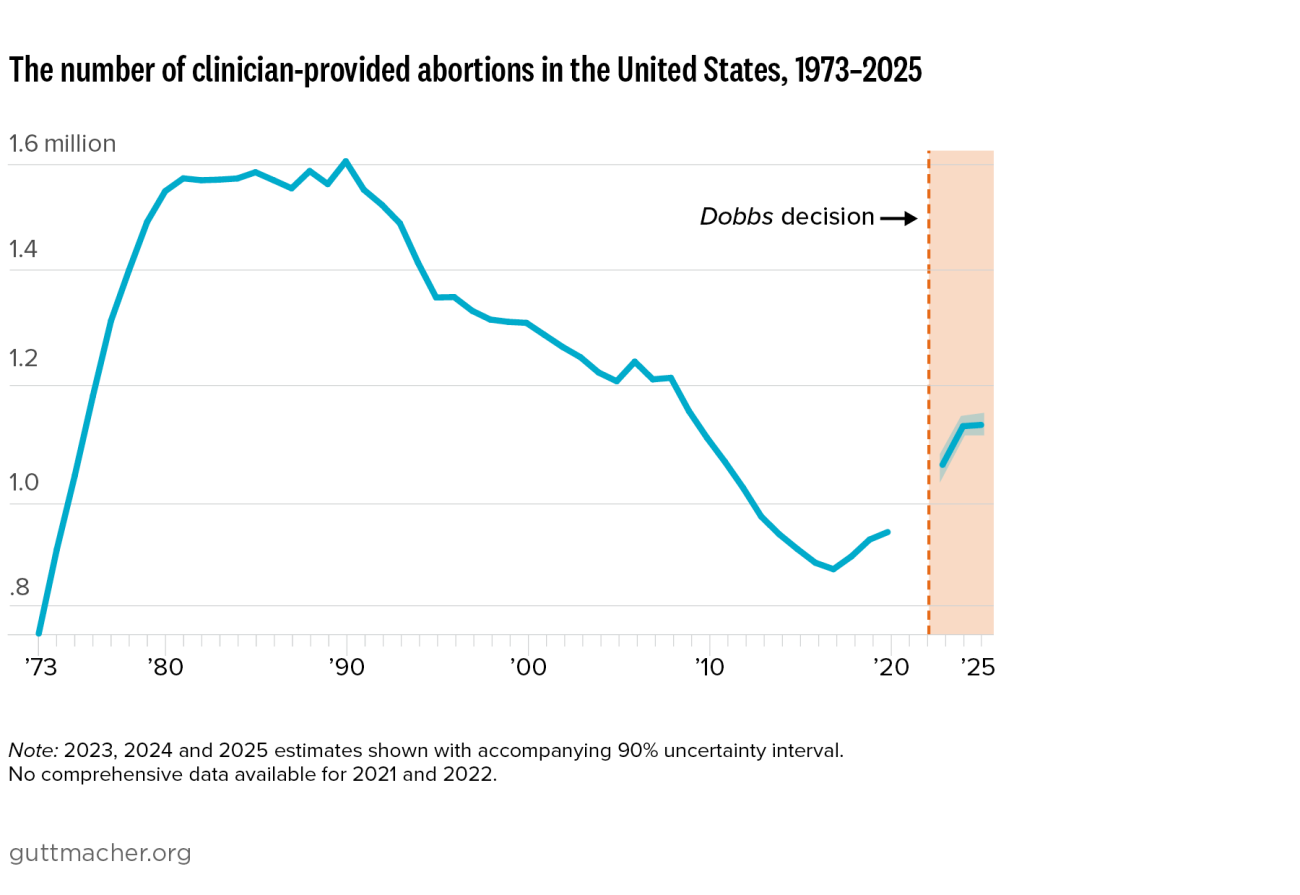
This report presents new 2025 full-year estimates of the incidence of clinician-provided abortion care and travel across state lines for abortion from Guttmacher’s Monthly Abortion Provision Study. For the first time, these include estimates of telehealth provision to residents of states with total bans; the report also updates prior year estimates to include these states.
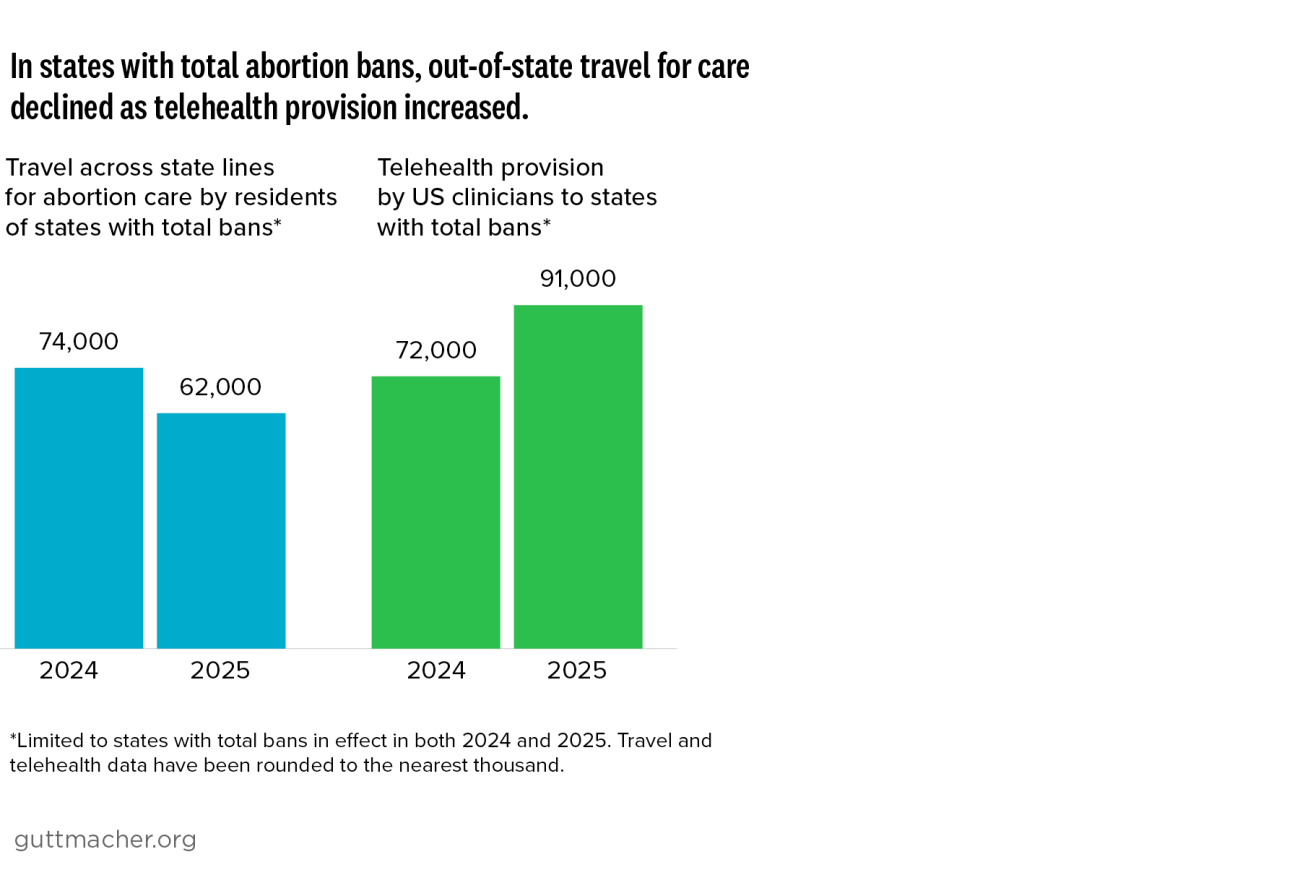
By the end of 2025, 13 states had total abortion bans (with limited exceptions) in effect, and six states had six- or twelve-week abortion bans. In addition, a series of blocked and reinstated abortion restrictions in Missouri created major obstacles for people seeking in-person care there, despite a 2024 state constitutional amendment protecting abortion rights. Many residents of states with severe restrictions or total bans obtained care via telehealth from providers in states with shield law protections while others traveled out of state for care.
Taken together, the estimates in this report paint a picture of ongoing shifts in how people—and particularly residents of states with total bans—are accessing abortion care as the US policy and provision landscape continues to change.