Key Points
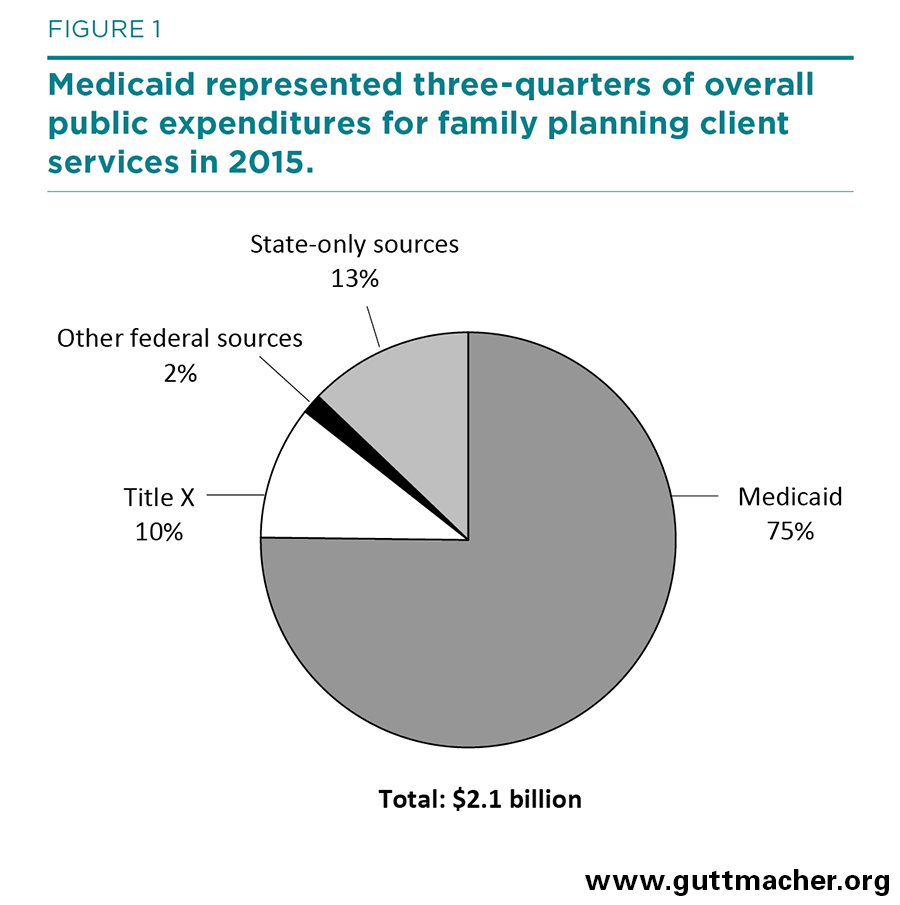
- Public expenditures for family planning client services totaled $2.1 billion in fiscal year (FY) 2015, supporting the provision of contraceptive drugs and devices, sterilization services, client counseling and education, and tests and treatment, including for STIs.
- Medicaid accounted for 75% of the total, state appropriations accounted for 13% and Title X accounted for 10%.
- Although total public funding in actual dollars has increased by more than $1.7 billion over the last 35 years, after adjusting for inflation, funding levels were essentially the same in FY 2015 as they were in FY 1980. However, reported FY 2015 expenditures appear to substantially undercount Medicaid expenditures.
- States spent $71 million on about 157,000 abortion procedures for low-income women in FY 2015, almost all of it in states that use their own funds to pay for most or all medically necessary abortions provided to Medicaid recipients. The federal government, which restricts funding to cases of life endangerment, rape and incest, contributed to the cost of only 160 of those procedures.