Key Points
- Seven in 10 U.S. women of reproductive age, some 44 million women, make at least one medical visit to obtain sexual and reproductive health (SRH) services each year.
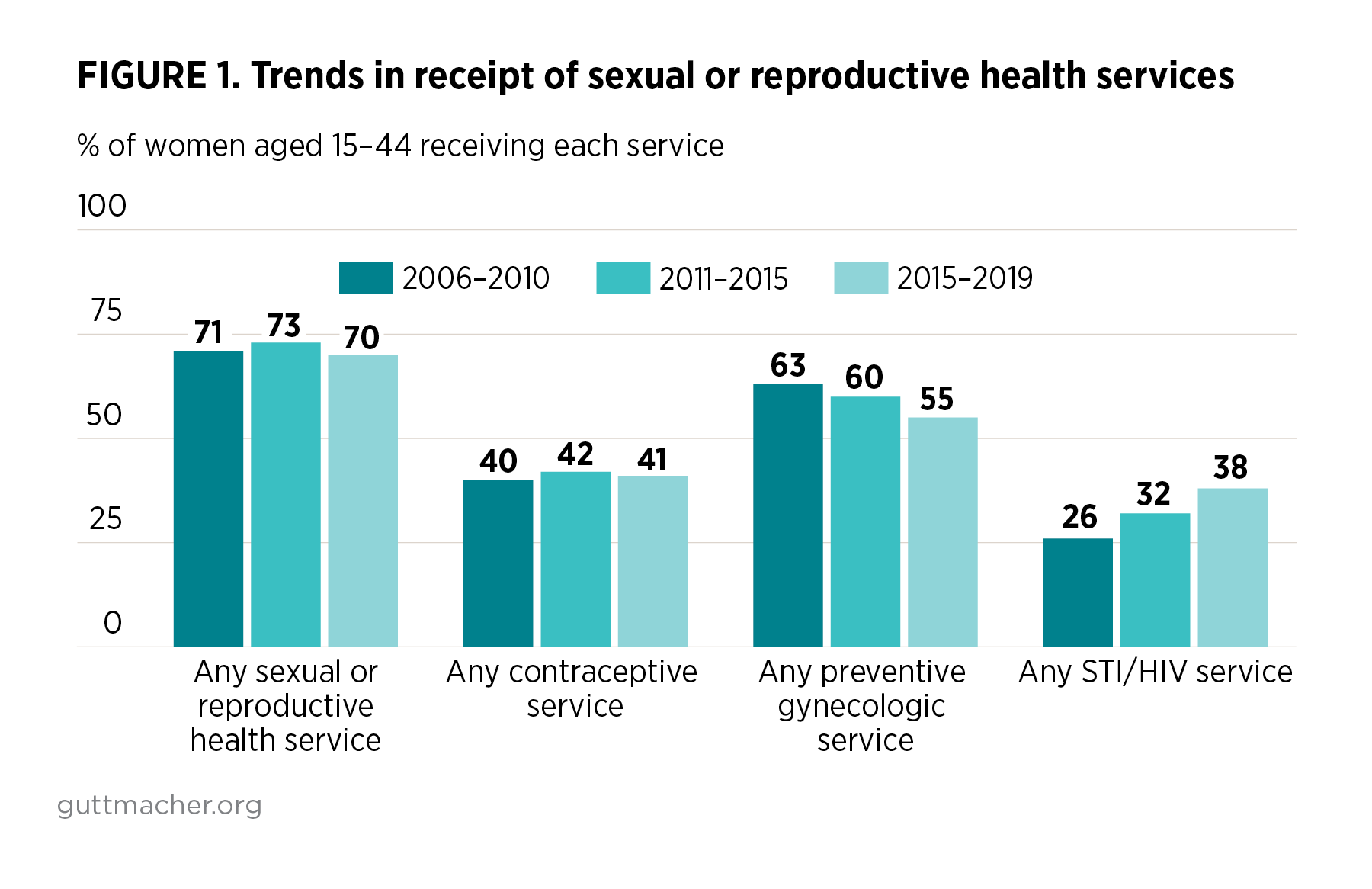
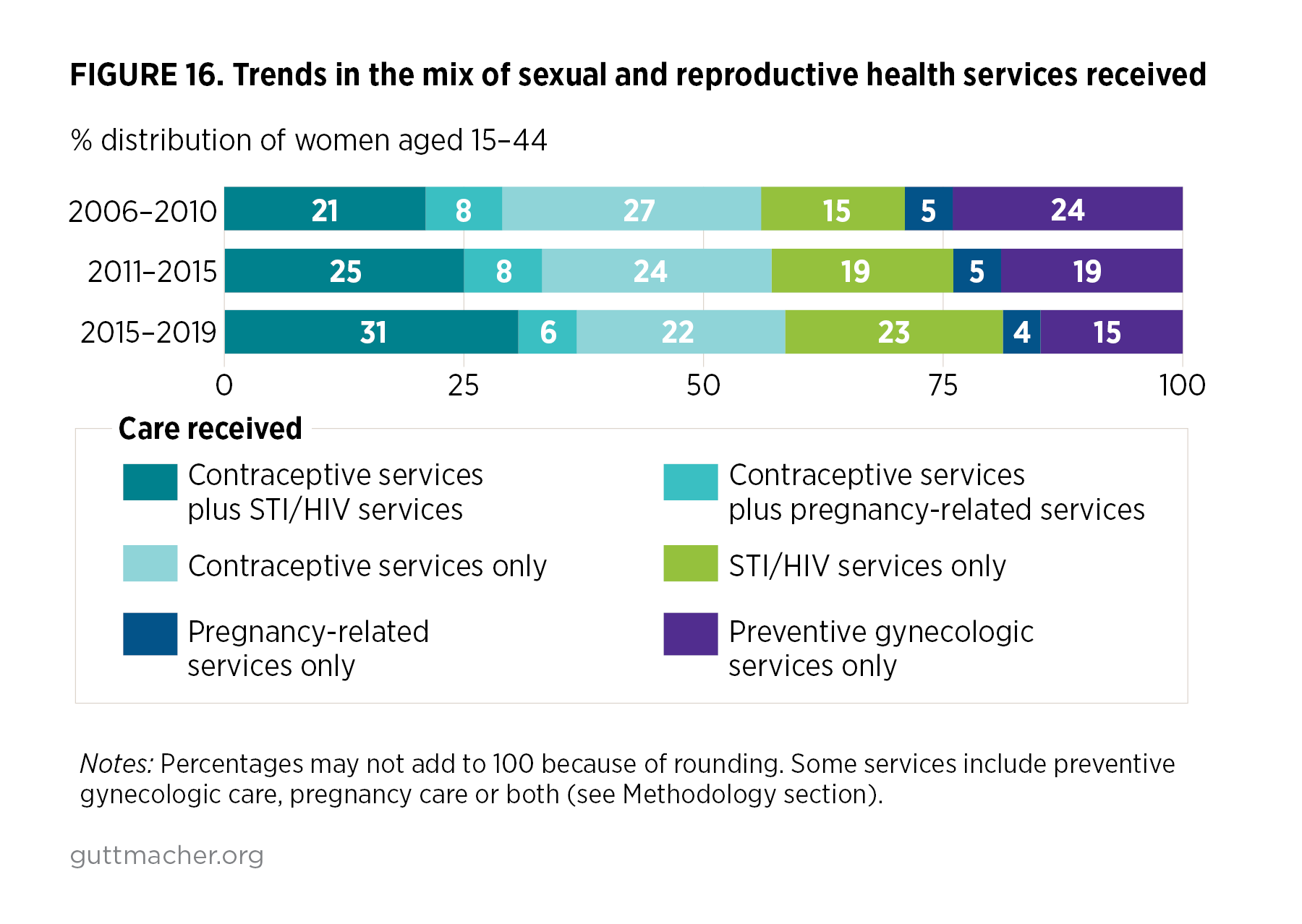
- While the overall number of women receiving any SRH service remained relatively stable between 2006–2010 and 2015–2019, the number of women receiving preventive gynecologic care fell and the number receiving STI testing doubled.
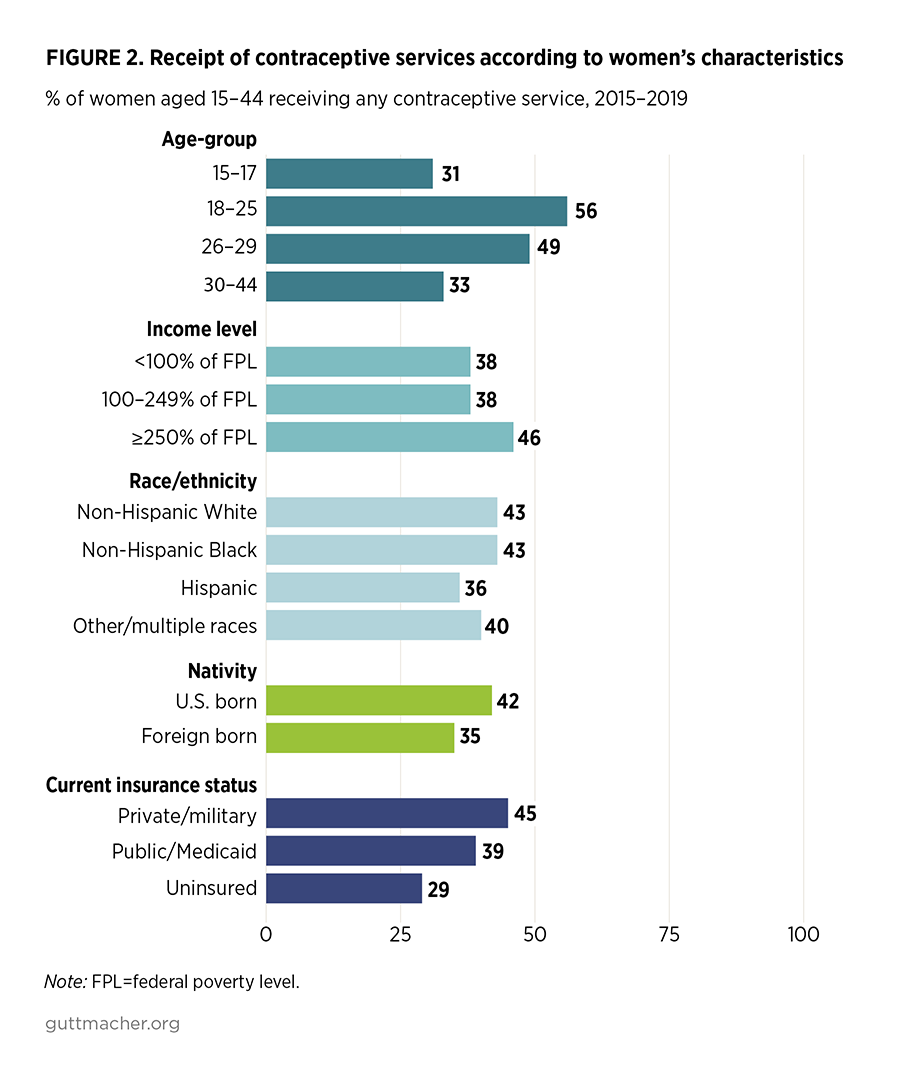
- Disparities in use of SRH services persist, as Hispanic women are significantly less likely than non-Hispanic White women to receive SRH services, and uninsured women are significantly less likely to receive services than privately insured women.
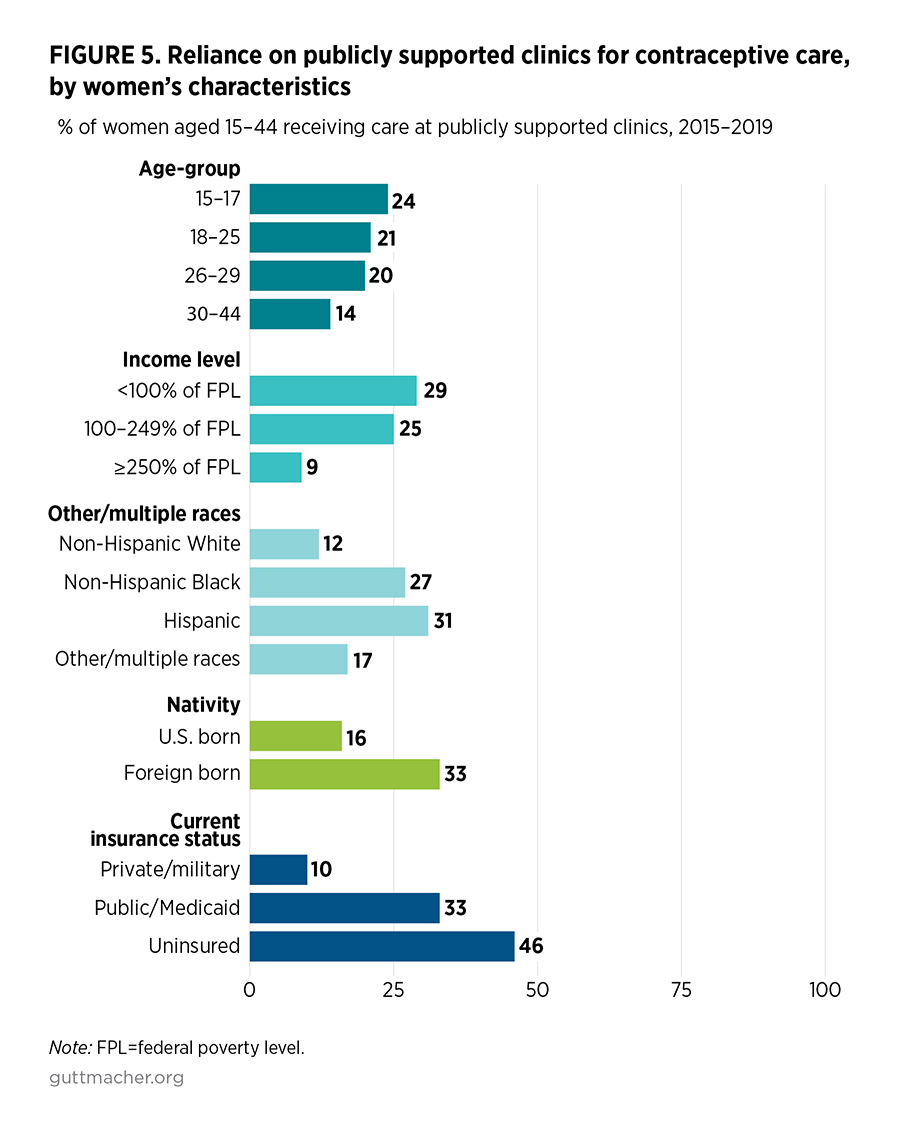
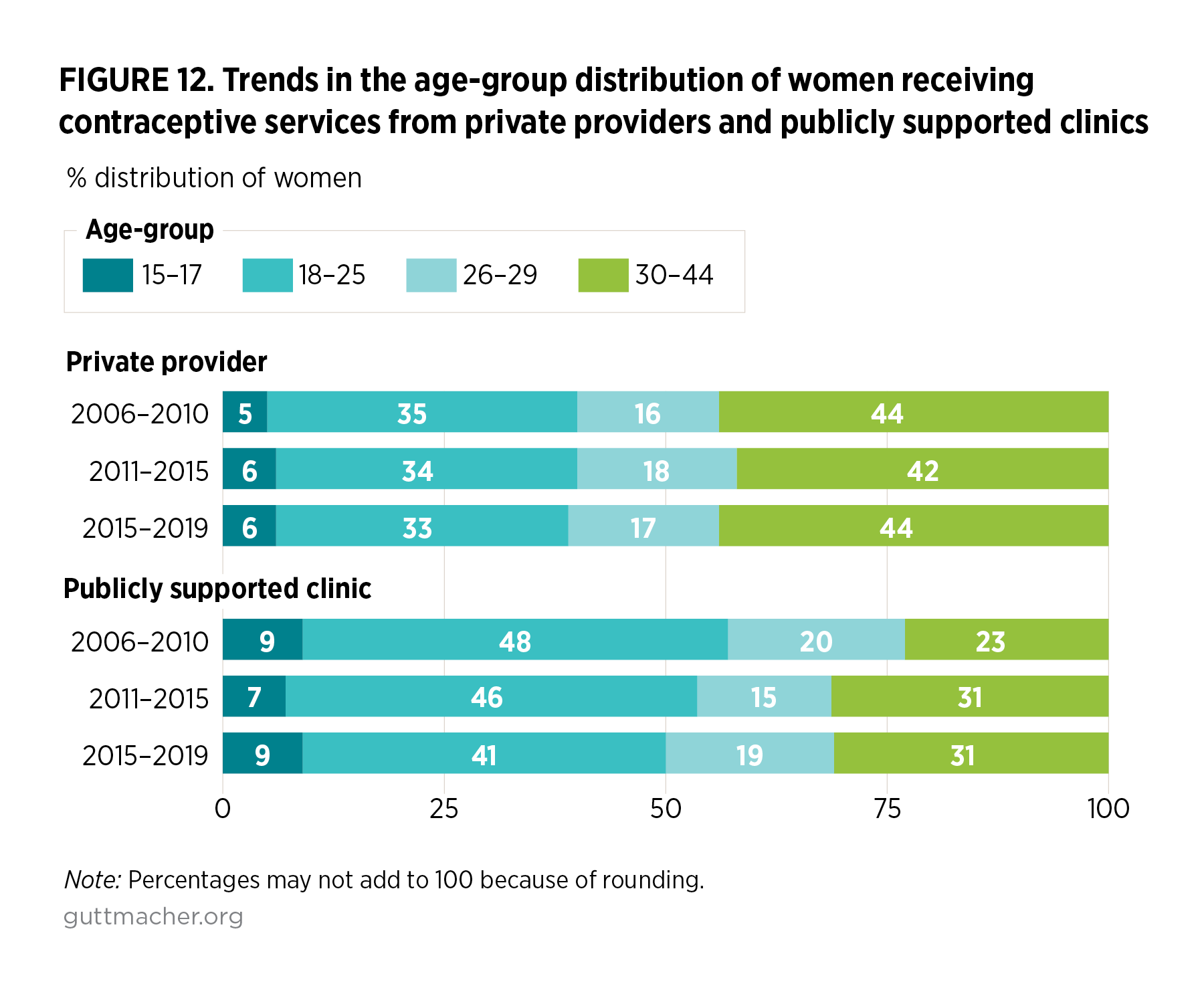
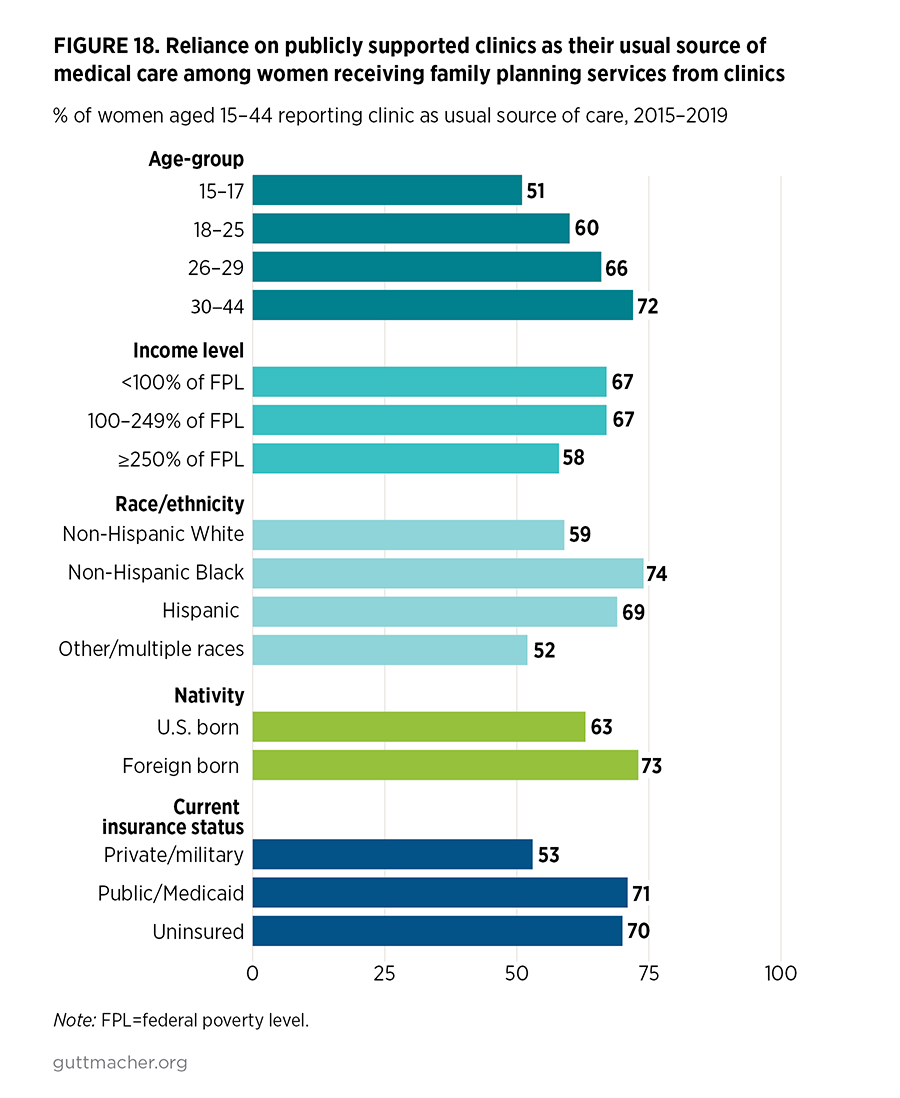
- Publicly funded clinics remain critical sources of SRH care for many women, with younger women, lower income women, women of color, foreign-born women, women with Medicaid coverage and women who are uninsured especially likely to rely on publicly funded clinics. Among women who go to clinics for SRH care, two-thirds report that the clinic is their usual source for medical care.
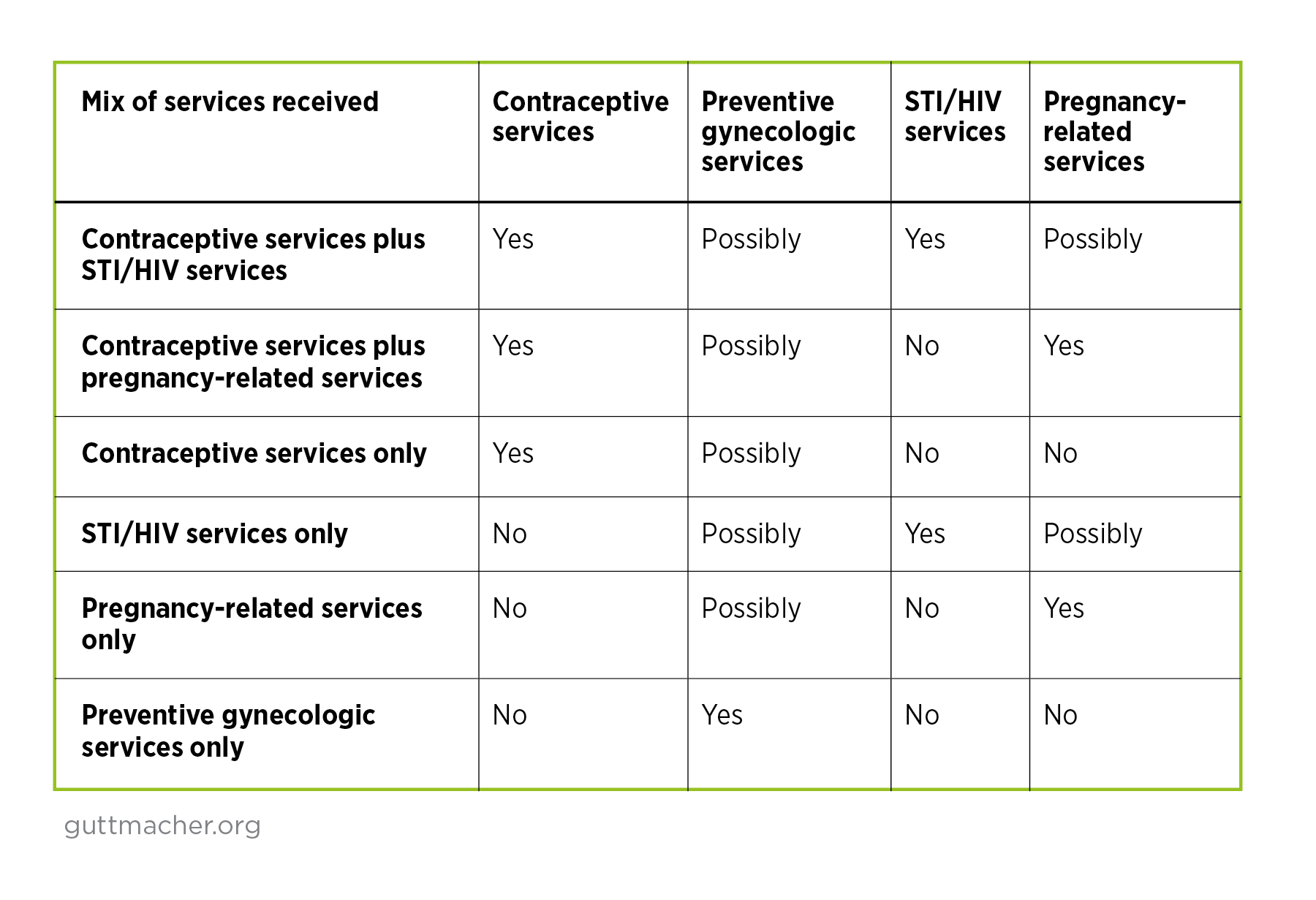
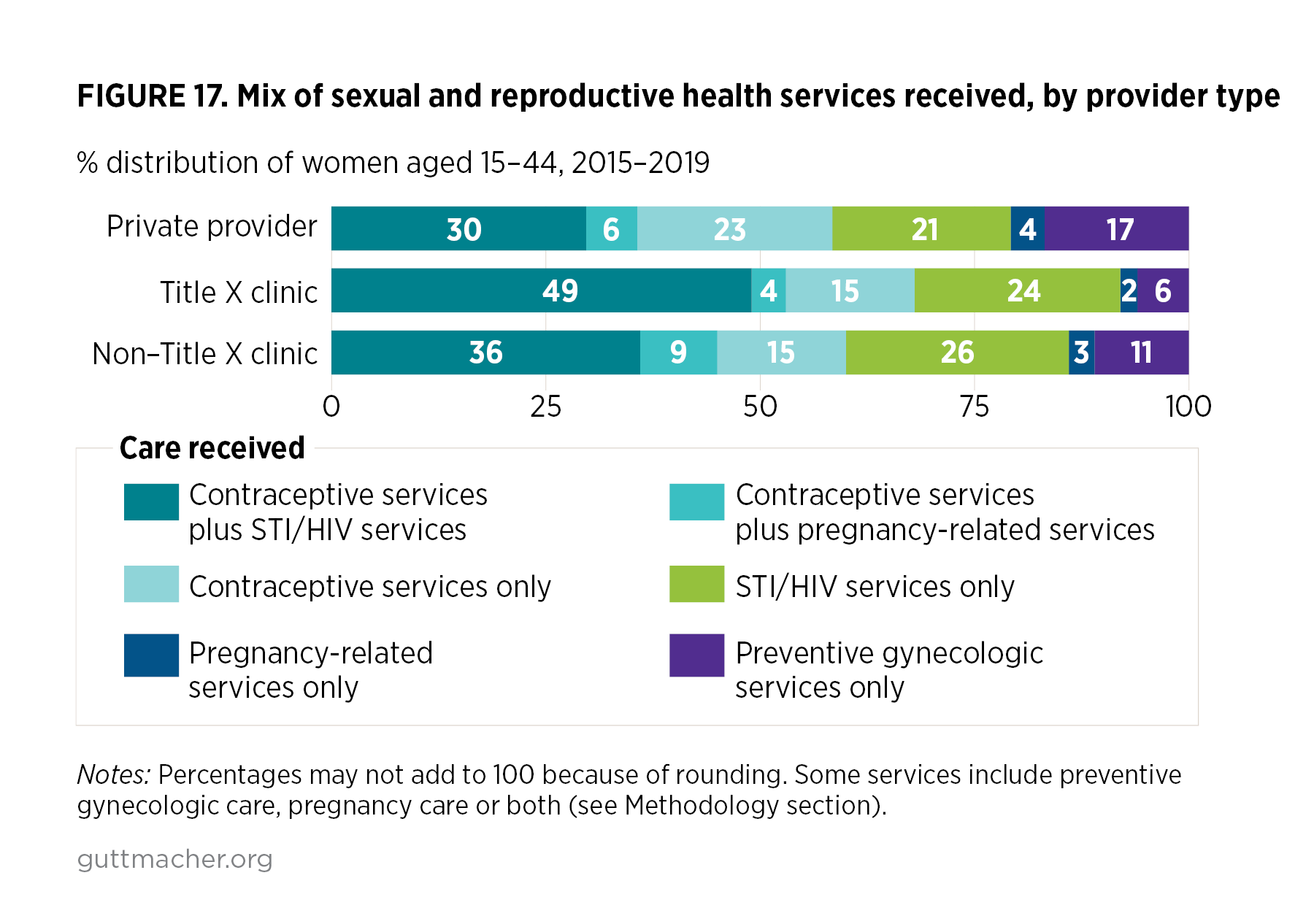
- Among those relying on both private providers and public clinics, the proportion of women who reported receiving a combination of contraceptive and STI/HIV care increased between 2006–2010 and 2015–2019.
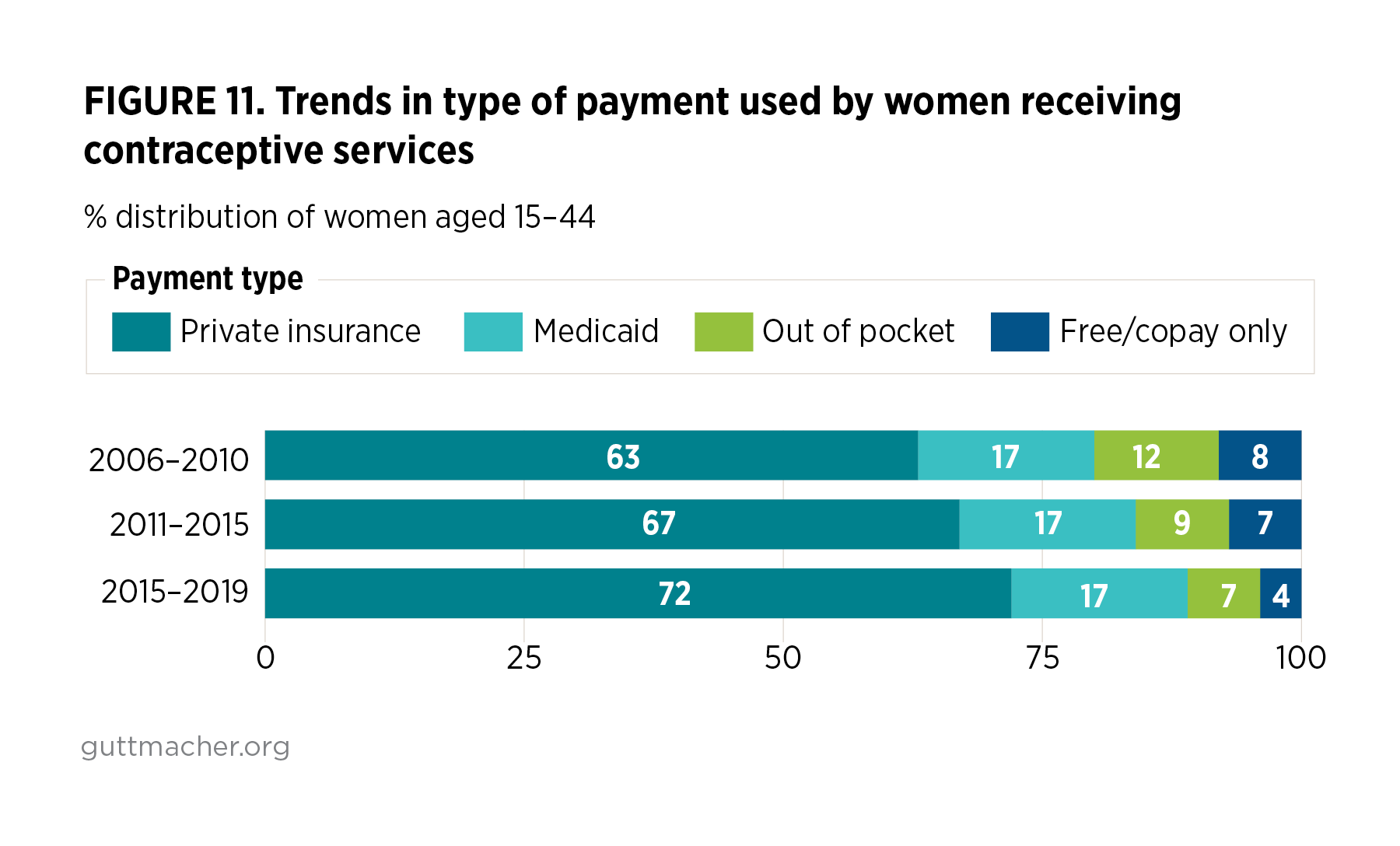
- Implementation of the Affordable Care Act has likely contributed to some of the changes observed in where women receive contraceptive and other SRH services and how they pay for that care:
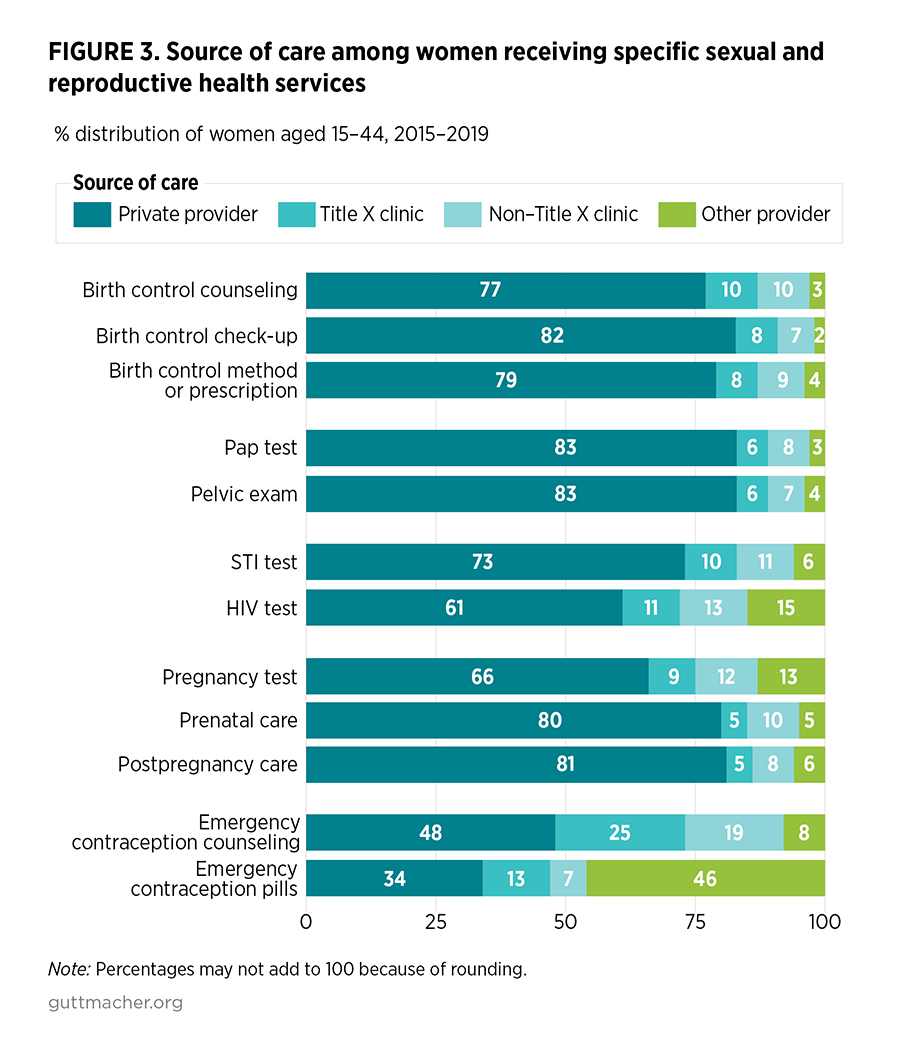
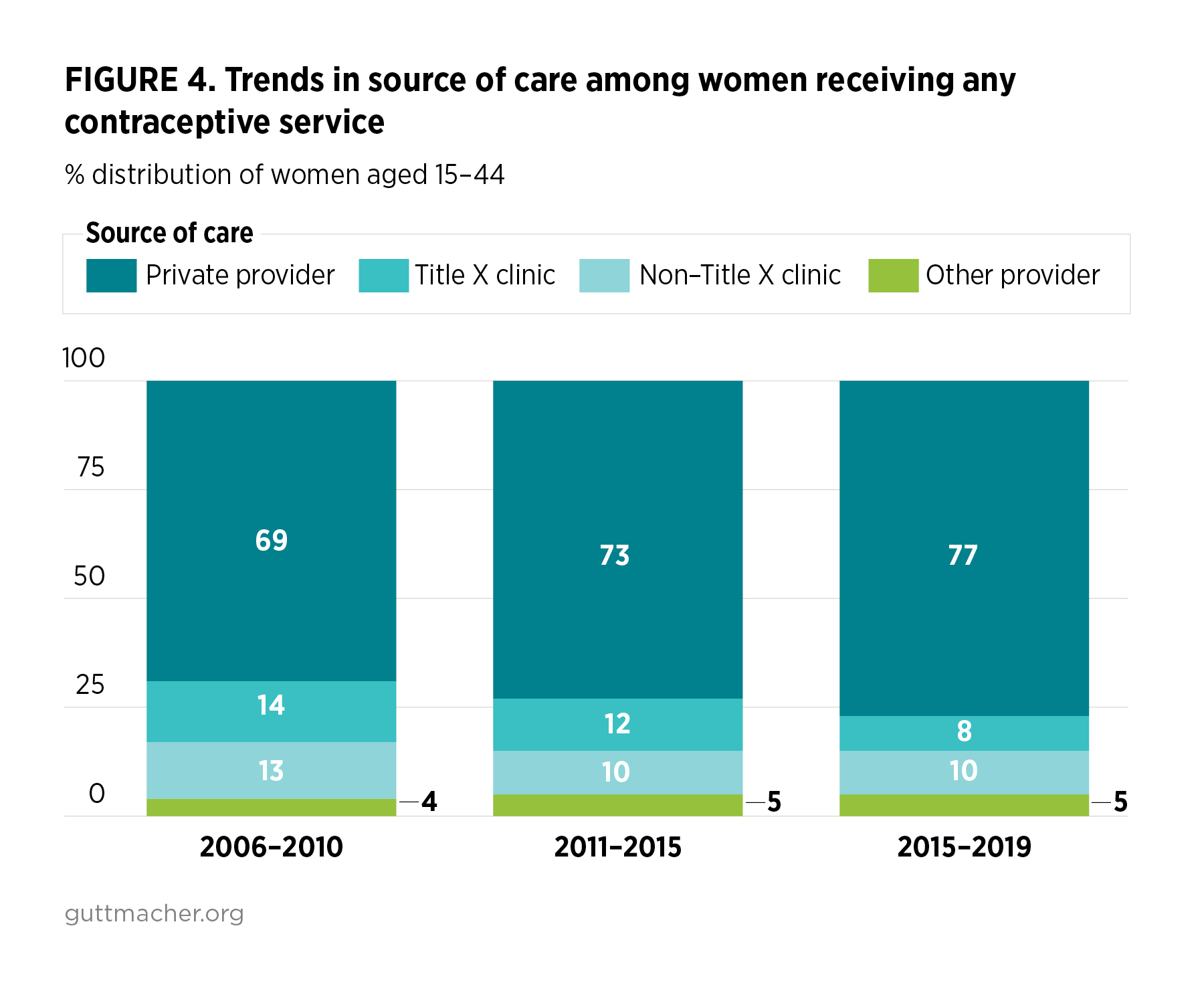
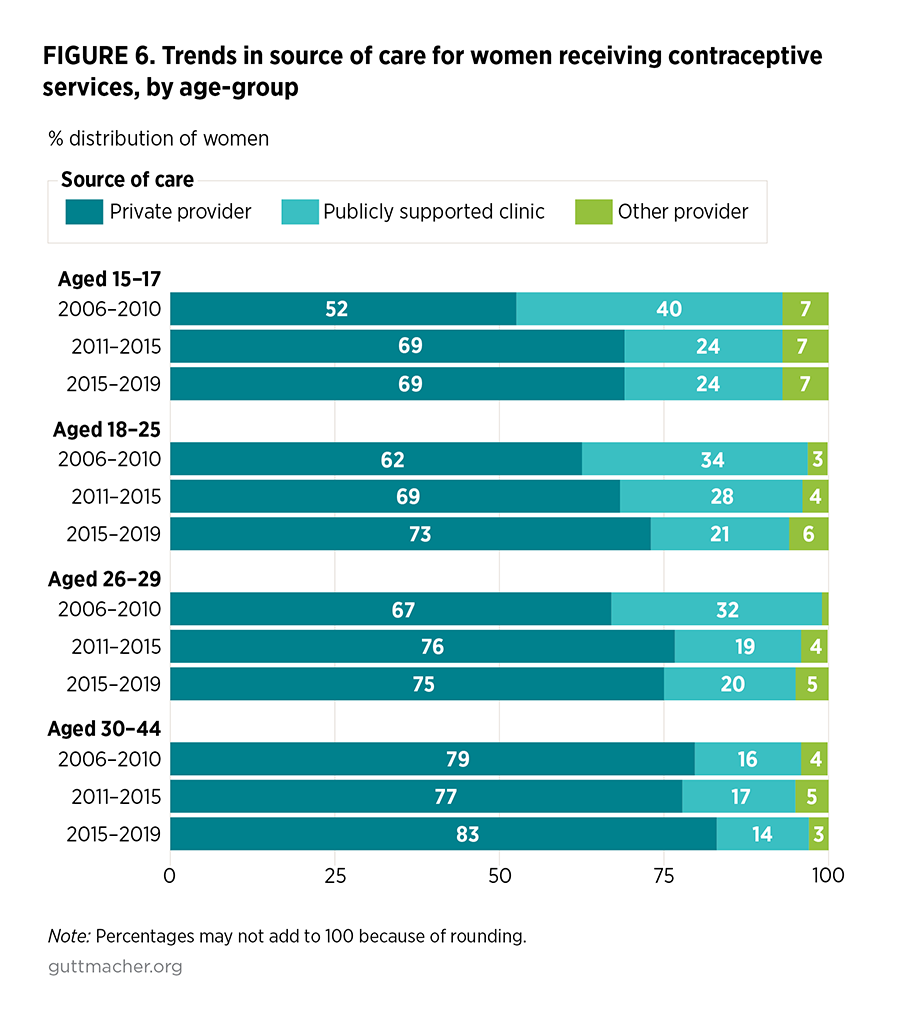
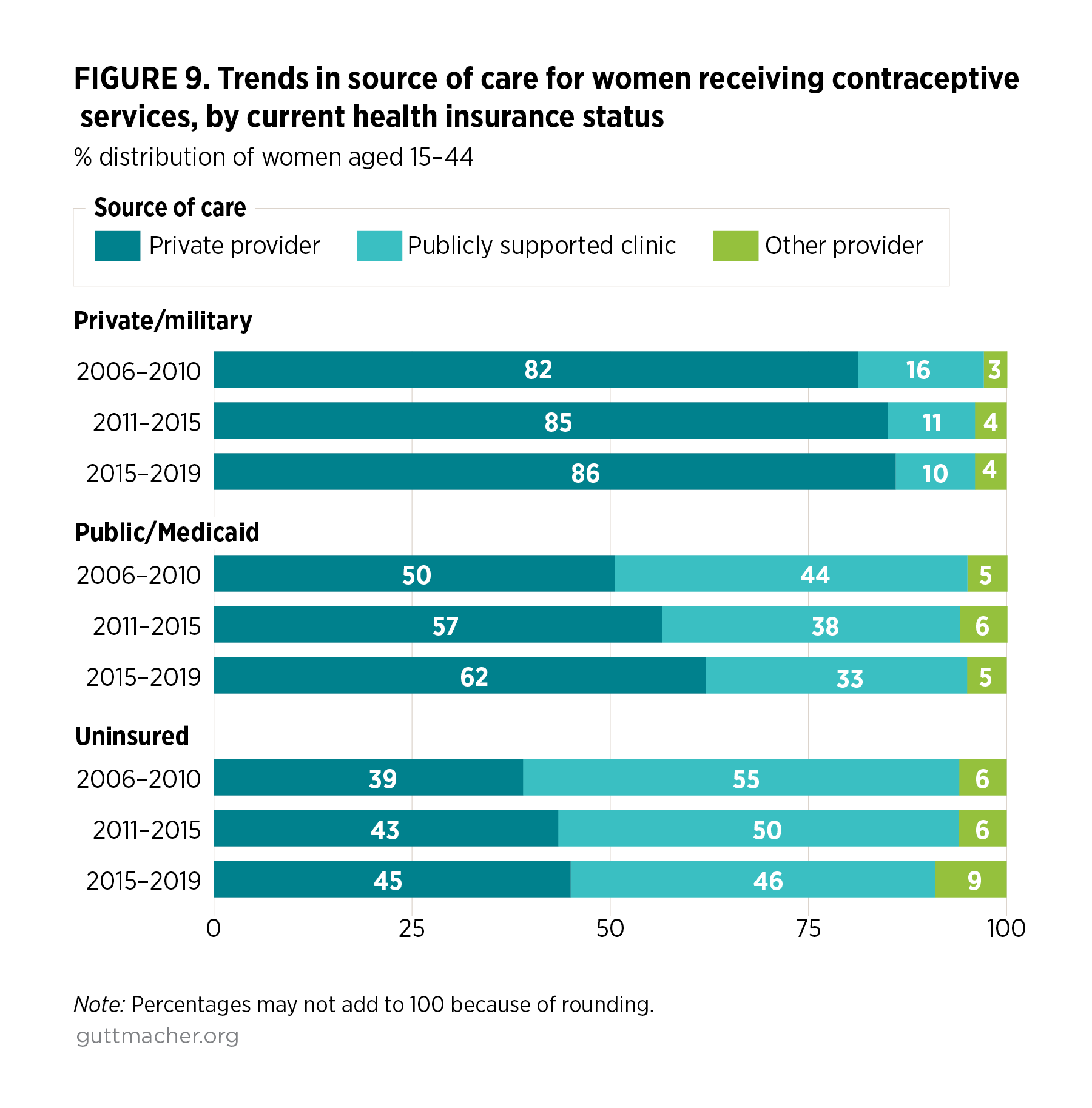
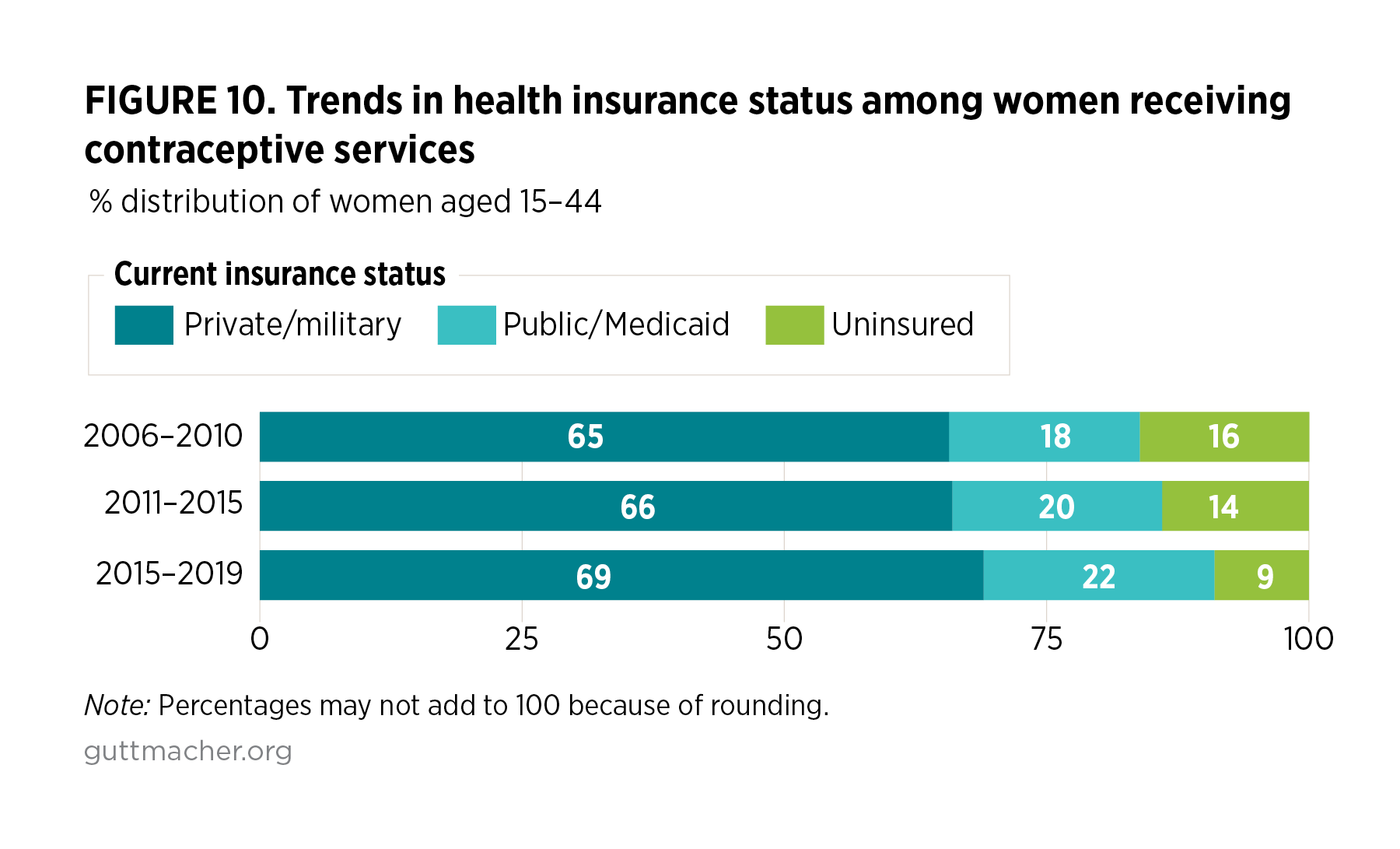
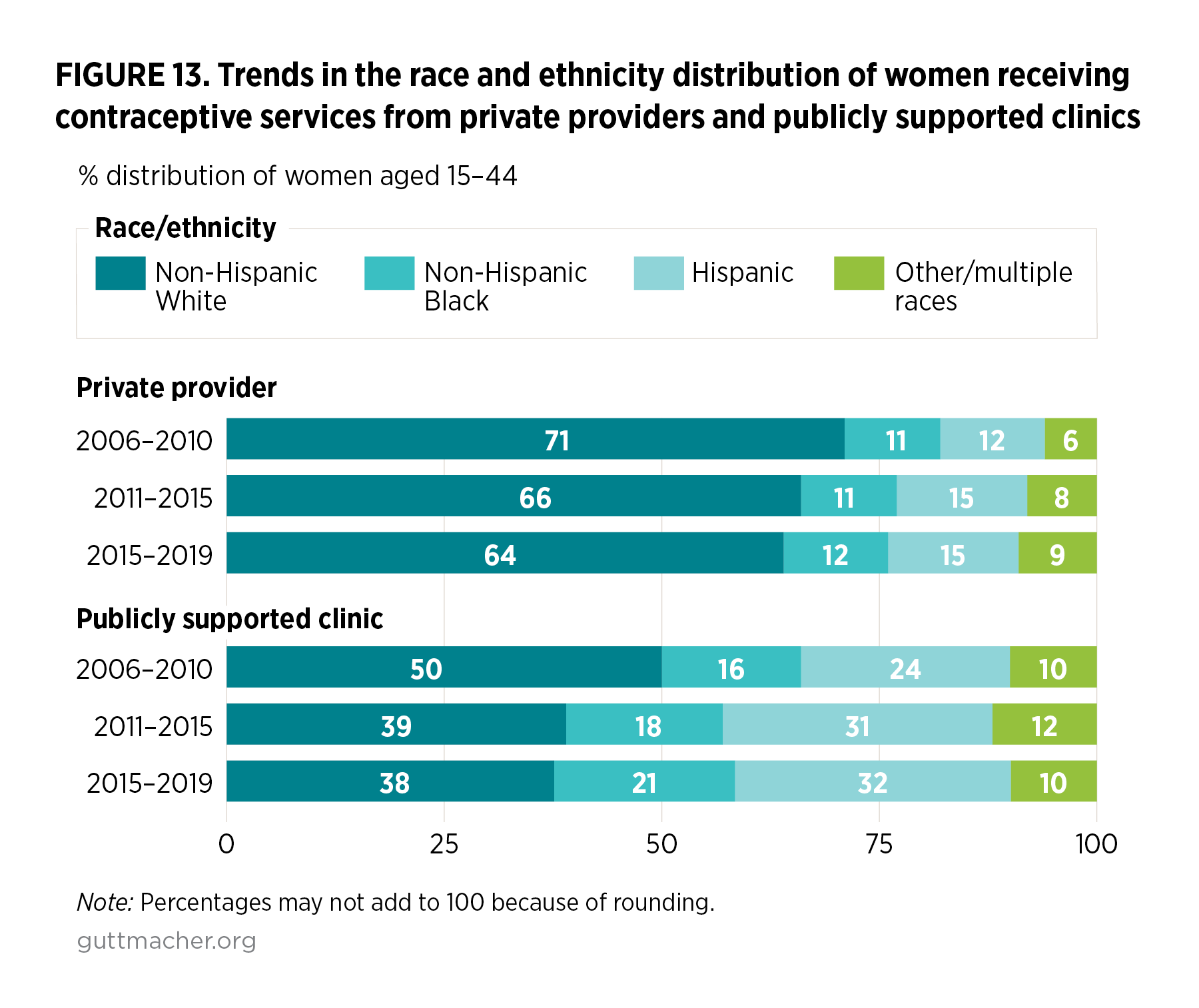
- The share of women receiving contraceptive services who go to private providers rose from 69% to 77% between 2006–2010 and 2015–2019, in part because more women gained private or public health insurance coverage and there was a greater likelihood that their health insurance would cover SRH services.
- There was a complementary drop in the share of women receiving contraceptive services who went to a publicly funded clinic, from 27% in 2006–2010 to 18% in 2015–2019.
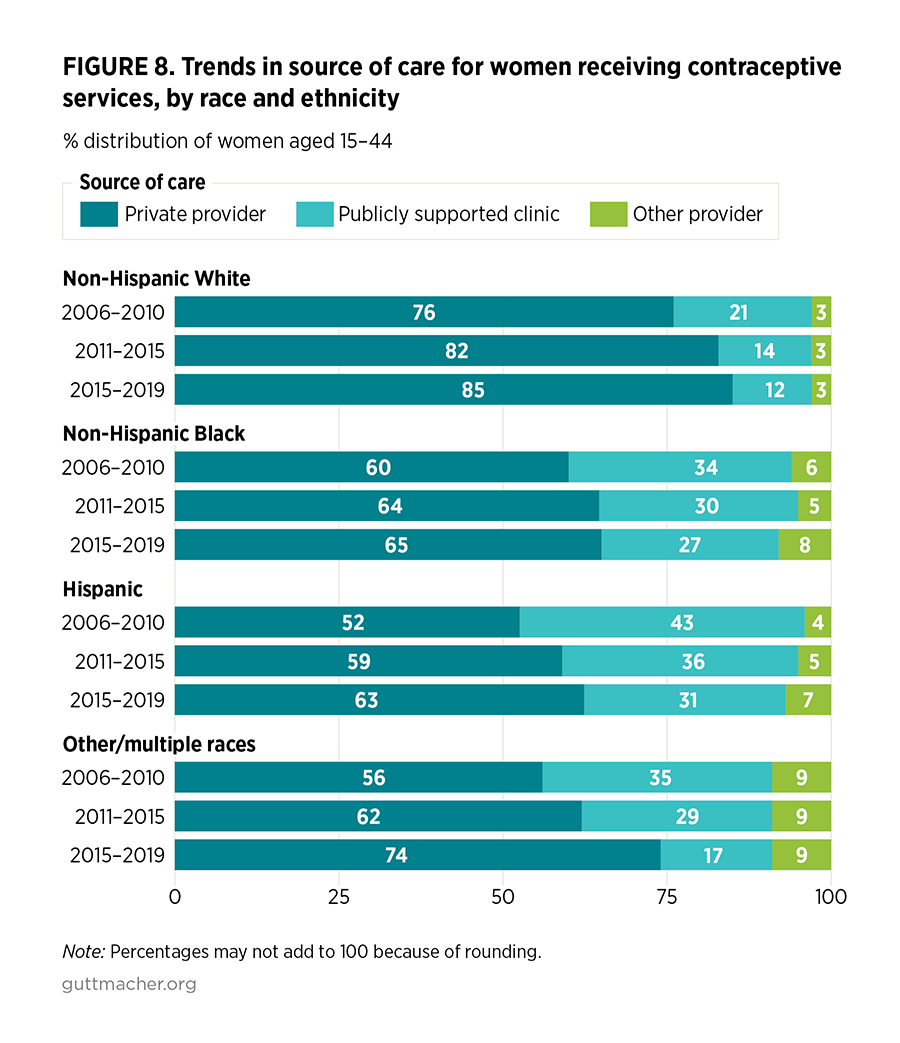
- For non-Hispanic Black women, immigrant women and uninsured women, there was no increase in the use of private providers for contraceptive care from 2006–2010 to 2015–2019.
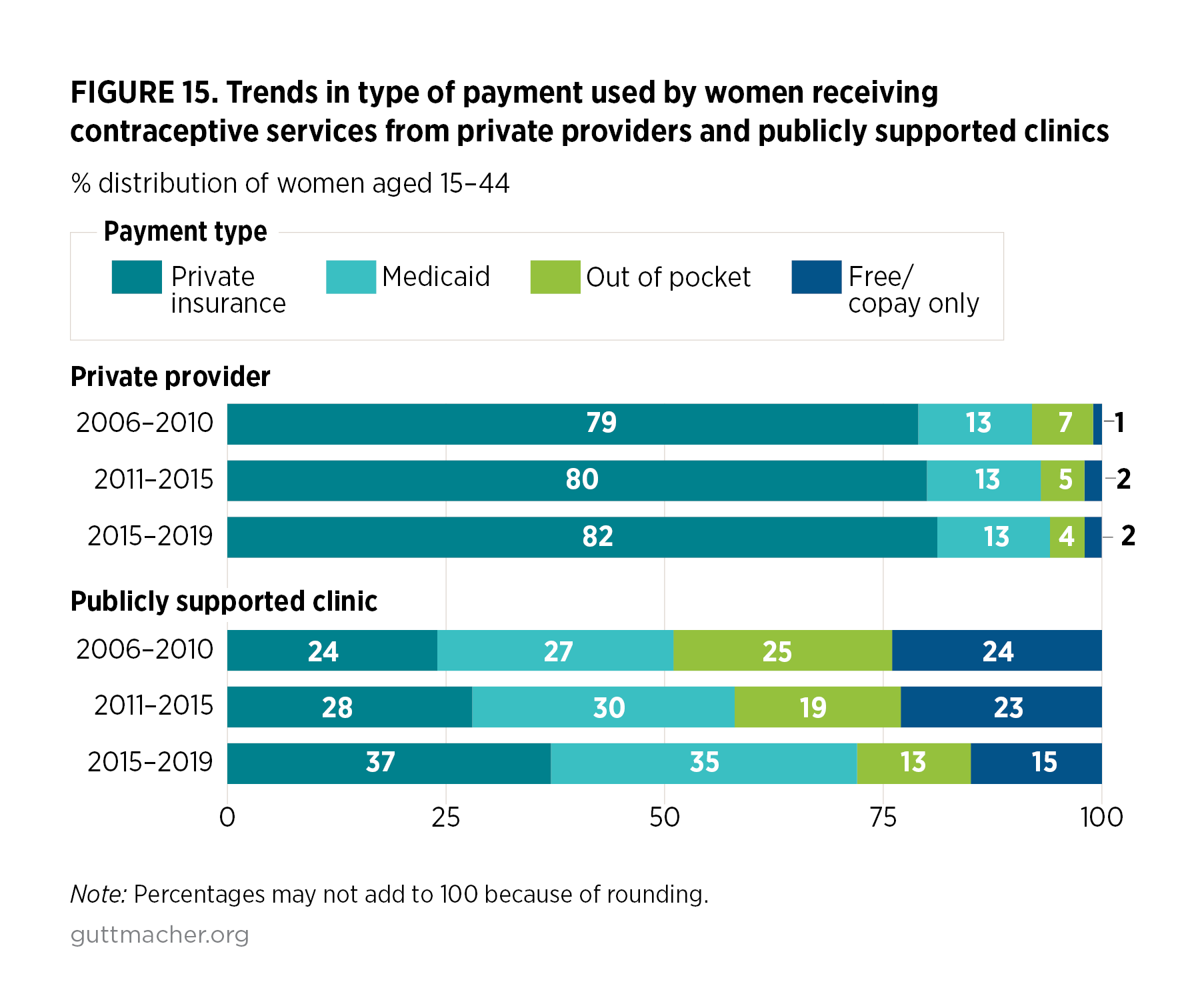
- Among women served at publicly funded clinics between 2006–2010 and 2015–2019, there were significant increases in the use of both public and private insurance to pay for their care.