In India, induced abortion is legal up to 20 weeks’ gestation, yet there are no state-level representative data on the health care services available to women seeking an abortion or care for complications following an abortion. This fact sheet examines the provision of these vital services in Gujarat.
Overview of the study
Between March and August of 2015, a team of researchers surveyed a sample of health facilities in six Indian states (Assam, Bihar, Gujarat, Madhya Pradesh, Tamil Nadu and Uttar Pradesh) as part of a study to generate high-quality data on the availability of induced abortion and postabortion care and the incidence of abortion and unintended pregnancy in India.
The study team randomly selected 70% of each state’s districts, and identified and sampled public, private and NGO facilities within these districts. In the public sector, district hospitals, subdivisional hospitals and community health centers (CHCs) were sampled using lists obtained from the Ministry of Health and Family Welfare (MOHFW). A portion of the primary health centers (PHCs) that are administratively linked to the sampled CHCs were also sampled. In addition, the study team listed and sampled public facilities not listed by MOHFW (urban public facilities), as well as private and NGO facilities (hospitals, medical colleges, maternity and nursing homes, and clinics) that offer induced abortion or postabortion services: In rural areas, facilities located in the catchment areas of a subsample of CHCs were listed, and in urban areas, facilities located within a sample of urban wards were listed. At each sampled facility, trained investigators conducted an in-person interview using a structured questionnaire with a senior professional knowledgeable about the provision of abortion-related services (typically the director or head of the facility or of the department responsible for obstetrics and gynecology). The study and its protocols were approved by the Institutional Review Boards of the three institutions conducting the study.
In Gujarat, 18 of 26 districts were sampled for inclusion in the study. A total of 262 public facilities (including 118 that reported providing any abortion-related service) completed the survey, as did 172 private facilities and five NGO facilities that provide abortion-related services. These represent all 1,561 public facilities operating in Gujarat (including 484 that provide abortion-related services), as well as the 1,811 private and NGO facilities offering abortion or postabortion care in the state. The analysis differentiates facilities according to ownership (public or private) and type (grouped into categories that generally correspond to facility capacity*). Because NGOs make up a very small proportion of our sample, they were combined with private facilities in this analysis. Detailed distributions in tables and figures do not always sum to 100 because of rounding.
Public and private facilities offering abortion-related services
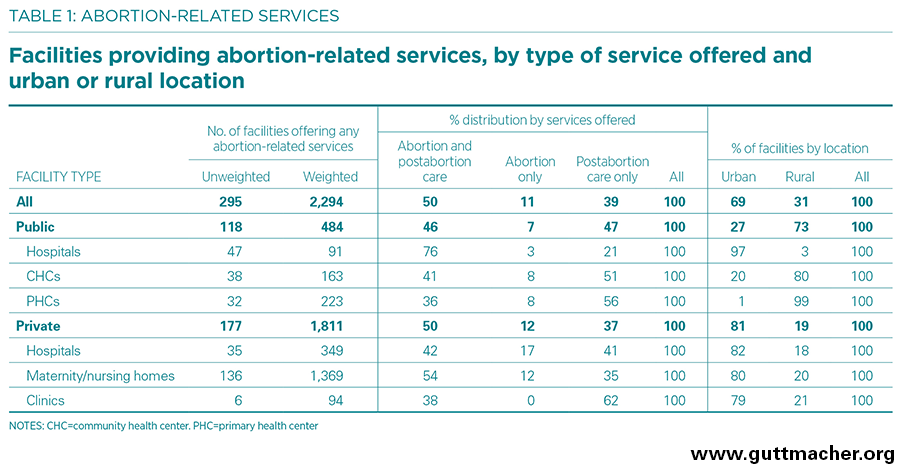
- An estimated 2,294 facilities in Gujarat provide abortion-related services (induced abortion, postabortion care or both; Table 1). Of these, 484 are public and 1,811 are private (including NGOs).
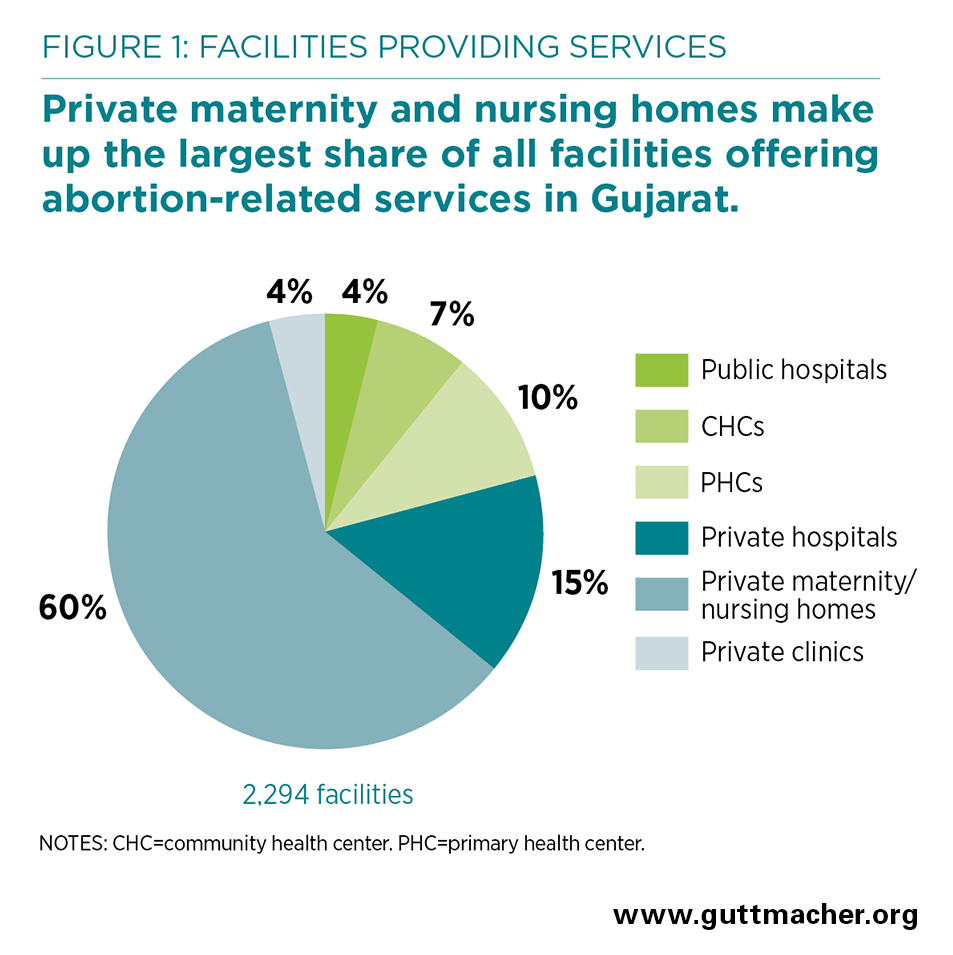
- Private maternity and nursing homes make up the largest share of all facilities offering abortion-related services, accounting for 60%, followed by private hospitals, which account for 15% (Figure 1).
- Among facilities offering any such services, 39% offer only postabortion care, 49% offer both abortion and postabortion care, and 11% offer only abortion.
- About three-fourths of public hospitals (76%) and slightly more than half of private maternity and nursing homes (54%) that offer any abortion-related services provide both types of care.
- In contrast, among PHCs and private clinics that offer any abortion-related services, the large majority (56–62%) provide only postabortion care.
- Two-thirds (69%) of facilities offering abortion or postabortion care are located in urban areas. Most of these urban facilities (92%) are privately owned.
- In rural areas, on the other hand, half of facilities that offer abortion-related services are public (50%).
- Among private facilities offering abortion, 87% report they are certified under the Medical Termination of Pregnancy Act to provide this service.
Availability of abortion-related services in the public sector
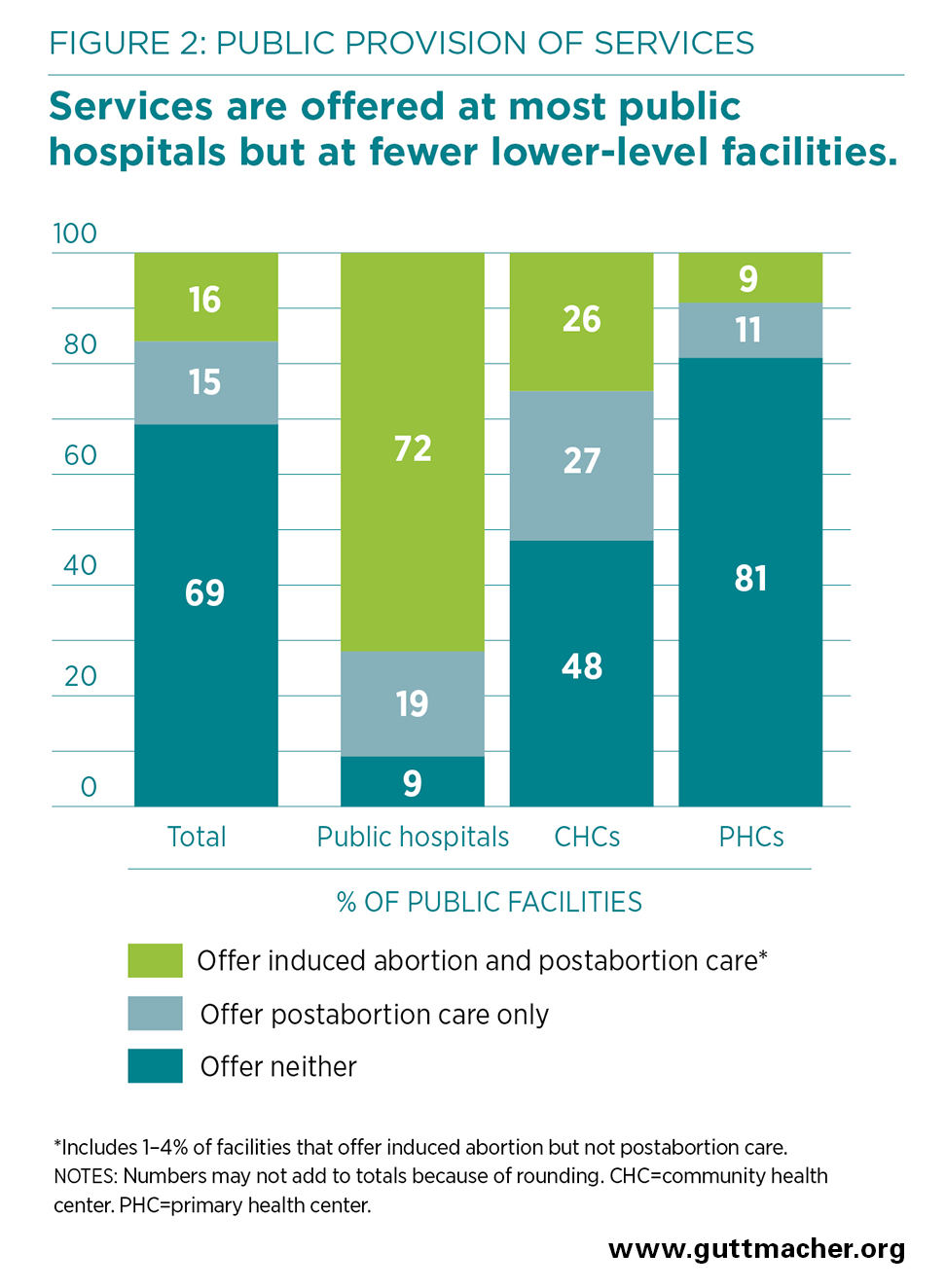
- Thirty-one percent of all public facilities in Gujarat offer some type of abortion-related services (Figure 2). Sixteen percent offer both abortion and postabortion care (including 2% that offer only abortion), while 15% offer only postabortion care. Sixty-nine percent of public facilities offer neither service.
- Public provision of abortion-related services varies by facility type: Most hospitals (91%) and 52% of community health centers (CHCs) offer abortion, postabortion care or both, whereas only 20% of PHCs do so.
- Sixteen percent of public facilities in Gujarat provide induced abortion—72% of hospitals, 26% of CHCs and 9% of PHCs—and almost all of these facilities also offer postabortion care (69% of hospitals, 21% of CHCs and 7% of PHCs offer both).
- Overall, 29% of public facilities provide postabortion care, and many offer only postabortion care: 19% of hospitals, 27% of CHCs and 11% of PHCs.
- Viewed another way, the data show that a large majority (84%) of public facilities—28% of hospitals, 74% of CHCs and 91% of PHCs—do not offer abortion.
Reasons for not offering abortion
- Among facilities whose abortion-related services are restricted to postabortion care, the reasons reported for not offering induced abortion vary according to whether facilities are public or private.
- Public facilities offering only postabortion care most commonly cite lack of trained staff (77%) and lack of equipment or supplies (44%) as reasons for not offering abortion.
- In contrast, private facilities offering only postabortion care most commonly report religious or social reasons (48%) or lack of certification (42%) as grounds for not offering the procedure; few private facilities report lack of trained staff (11%) or lack of equipment or supplies (11%).
- Among all public facilities not offering abortion—including those that offer no abortion-related services, as well as those offering only postabortion care—the most prevalent reasons reported for not doing so are the same as those reported by public facilities offering only postabortion care: lack of trained staff (81%) and lack of equipment or supplies (46%).
- Reasons vary by type of public facility. Among all public hospitals not offering abortion, lack of trained staff is the main reason cited (81%), followed by religious or social reasons (19%). CHCs and PHCs cite lack of trained staff (72–83%), equipment or supplies (34–50%) and space (11–18%) as the main reasons for not providing abortion.
Types of abortion procedures offered
- Among the public and private facilities that provide induced abortion services, 76% offer both medical methods of abortion (MMA)† and surgical methods, 12% offer only MMA and 12% offer only surgical methods.
- Facilities offering abortion report using the following specific methods: MMA using combipacks containing misoprostol and mifepristone (offered by 88%); MMA using only misoprostol (33%); manual vacuum aspiration (MVA) or electric vacuum aspiration (EVA) procedures (69%); and dilatation and evacuation or dilatation and curettage (83%).
- A higher proportion of private facilities (80%) than of public facilities (59%) that offer abortion use both MMA and surgical methods.
- Sizable shares of lower-level facilities that offer abortion report that provision is limited to MMA: 38% of CHCs, 35% of PHCs and 49% of private clinics.
Vacuum aspiration equipment and training
- In Gujarat, nearly all facilities that offer abortion using MVA or EVA (94–98%) have functional equipment available at least some of the time and at least one provider trained in the procedure.
- A somewhat lower proportion (80–92%) of facilities offering these procedures have a trained provider and have functional equipment available all or most of the time when it is needed. This proportion is lowest among PHCs offering MVA (69%).
Gestation at which abortion services are offered
- In India, abortion is legal up to 20 weeks’ gestation; for abortions performed between 12 and 20 weeks, authorization by two doctors is required. Pregnancies beyond 20 weeks may be terminated only to save a woman’s life.
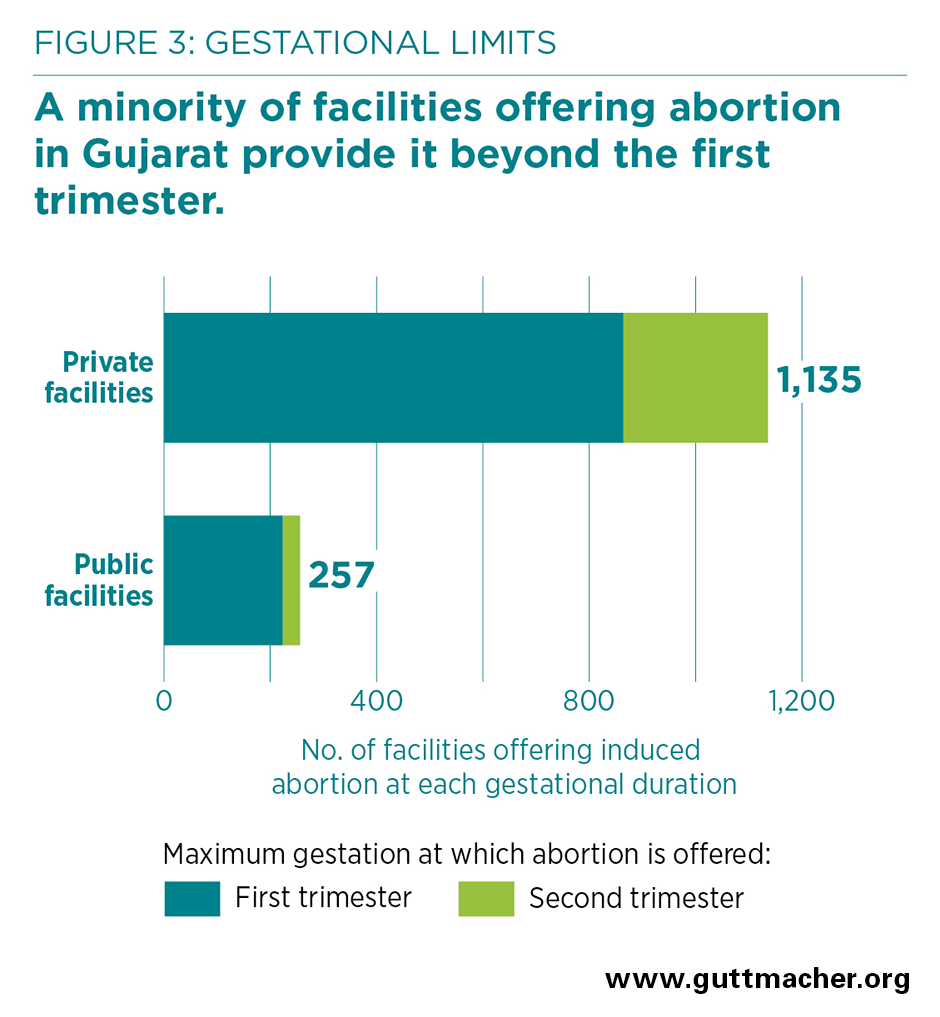
- However, the large majority of facilities providing abortion services in Gujarat—78%—offer procedures during the first trimester only (at or before 12 weeks); 25% of facilities restrict provision to the first seven weeks of pregnancy. All CHCs and PHCs that offer abortion do so only in the first trimester.
- Among the 1,135 private facilities offering abortion, 24% provide services during the second trimester of pregnancy (Figure 3). Among the 257 public facilities offering such care, only 13% provide second-trimester procedures.
- Although abortion provision beyond the first trimester is relatively inaccessible throughout the state, the proportion of facilities offering second-trimester procedures is particularly low in rural areas (4%), compared with urban areas (28%).
Consent for abortion procedures
- Providers are required to obtain a woman’s consent before performing an abortion, and nearly all facilities (98%) report this is commonly done.
- Consent is not legally required from anyone other than the woman obtaining the procedure, unless she has a mental illness or is a minor. However, many facilities (71%) routinely seek the consent of the woman’s husband or partner. Thirteen percent report commonly asking for consent from married women’s in-laws, and 8% report commonly asking the parents of unmarried women.
Turning away abortion seekers
- Overall, an estimated 8% of women seeking induced abortion from facilities offering abortion in Gujarat were turned away.
- More than half (56%) of facilities offering induced abortion report having turned away one or more women seeking an abortion in the last year. Among these facilities, the most common group of reasons for turning away abortion seekers was related to capacity to provide needed abortion services—including that the pregnancy was too far along for the facility or that the facility lacked a trained provider (57% of facilities that turned away any abortion seekers reported one or both of these reasons).
- Facilities also report turning away some women who could have been served. Slightly over one-third (37%) of facilities that turned away women seeking abortion did so for one or more of the following reasons: the woman was "too young," had no children or was unmarried. A small proportion of facilities that turned away abortion seekers (13%) did so because the woman’s husband or partner had not consented to the procedure.
Accessibility of postabortion care
- Eighty-five percent of facilities providing postabortion care services (including more than 95% of public and private hospitals) offer care 24 hours a day, seven days a week.
- Availability of around-the-clock postabortion care is greater among facilities providing this care in urban areas (90%) than among those in rural areas (76%). In rural areas, care is available 24-7 at 100% of public hospitals and 83% of CHCs, but at only 57% of PHCs.
- Seventy-four percent of facilities offering postabortion care services provide both outpatient and inpatient care. However, 17% of public facilities and 15% of private facilities offer only outpatient services, indicating that they may not have the capacity to treat severe complications.
- One-third of PHCs (31%) and nearly two-thirds of private clinics (60%) offer only outpatient services.
Contraceptive care offered
- Nearly all facilities in Gujarat that offer abortion-related care report providing information about family planning to the vast majority of women seeking induced abortion or postabortion care services.
- Although most of these facilities cover the advantages and disadvantages of different methods (70%) and the correct use of methods (56%), fewer provide information on what methods are available (38%) or what to do in case of method failure or incorrect use (19%). These proportions are similar at both public and private facilities.
- Nearly all facilities that offer abortion or postabortion care also provide contraceptives. However, facilities report that, on average, only about half of women seeking abortion-related services adopt a contraceptive method. Although contraceptive uptake is roughly comparable across most types of facilities (53–61%), it is somewhat lower at private clinics (31%).
- Twenty percent of facilities (31% of public facilities and 18% of private facilities) that offer any abortion-related services report that at least some women are required to adopt contraception as a condition of receiving an abortion.