This publication has been updated. Please see here for the latest version.
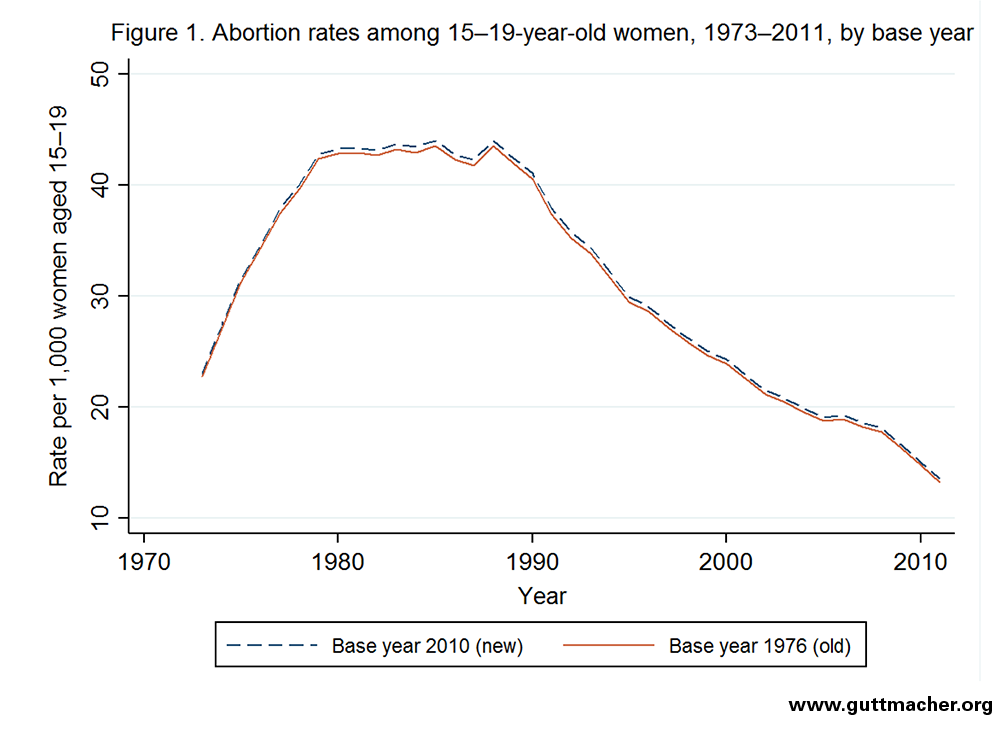
This report contains statistics for 2011 on the incidence of teenage pregnancy, birth and abortion for the United States as a whole, with trends since 1973. The report concludes with a discussion of the methodology and sources used to obtain the estimates.