For decades, Medicaid has been central to contraceptive care and other reproductive health services for low-income people in the United States. Massive cuts to Medicaid under the recent federal budget law are poised to strip away coverage and access to care from millions of people, with far-reaching and harmful consequences nationwide.
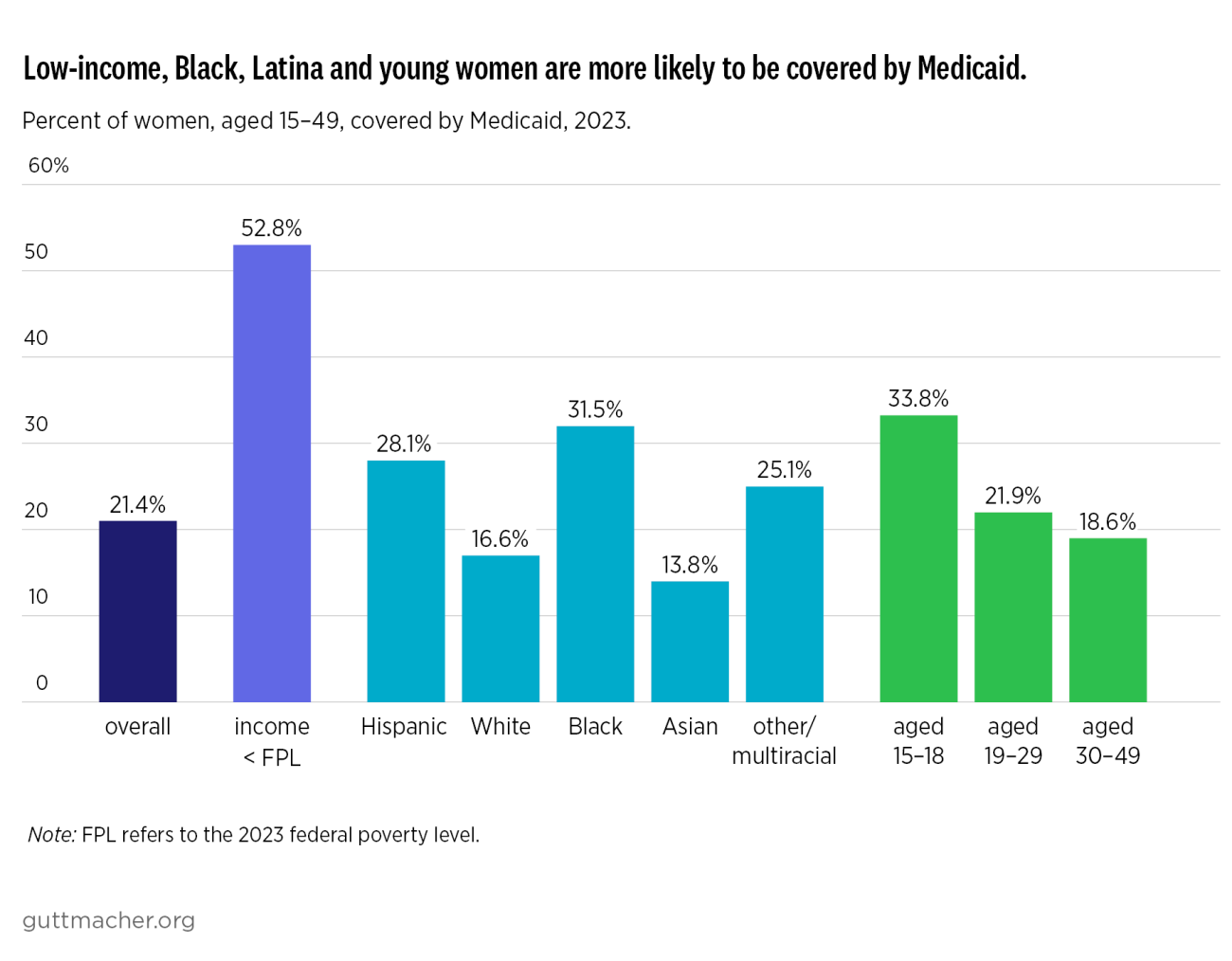
Medicaid is the second largest source of health insurance in the United States, and it covers 21% of women aged 15–49,* the group most likely to need and use reproductive health care. The program’s role has increased substantially over the past decade after 40 states and the District of Columbia expanded Medicaid for adults with incomes up to 138% of the federal poverty level, as allowed by the Affordable Care Act (ACA).
Under federal Medicaid law, states are required to cover family planning services and supplies without any out-of-pocket costs for enrollees. In addition, 31 states have expanded eligibility just for family planning services to people ineligible for full-benefit Medicaid coverage. As a direct result of these policies, 23% of US women rely on Medicaid to pay for contraceptive care, including 52% of those with incomes below the poverty level, according to unpublished tabulations from the National Survey of Family Growth (NSFG). At last count, Medicaid contributed 75% of all public dollars spent on family planning care and it covers 41% of all US births.