
Please note: All counts of enacted laws are current as of January 2, 2019.
Conservatives now have a clear majority on the U.S. Supreme Court and Roe v. Wade is in jeopardy of being hollowed out or overturned. Against that backdrop, policymakers in a number of states continued to pass new abortion restrictions in 2018, including measures clearly intended to violate Roe by banning abortion at early stages of pregnancy. At the same time, more than half of all states adopted measures to expand or protect access to sexual and reproductive health care.
Challenging Roe
Cases from previous years challenging the fundamental right to abortion are already on the Supreme Court’s doorstep. Indiana has asked the Court to uphold a state law that bans abortion for purposes of race or gender selection or genetic anomaly, or procedures based on the fetus’s color, national origin or ancestry; the law also includes unnecessary and burdensome requirements related to the disposal of fetal tissue following an abortion. Alabama has asked the Court to review the state’s ban on the most common method of abortion used after 12 weeks of pregnancy.
Conservative state policymakers, particularly since 2010, have been deliberately passing laws that are designed to draw lawsuits challenging their constitutionality and provide opportunities for at least one of these cases to reach a Supreme Court interested in rolling back abortion rights. The 424 abortion restrictions enacted in just the last eight years comprise more than a third of all abortion restrictions enacted since Roe was decided in 1973. Although some have been challenged in court, most are in effect.
Trends in State Legislation
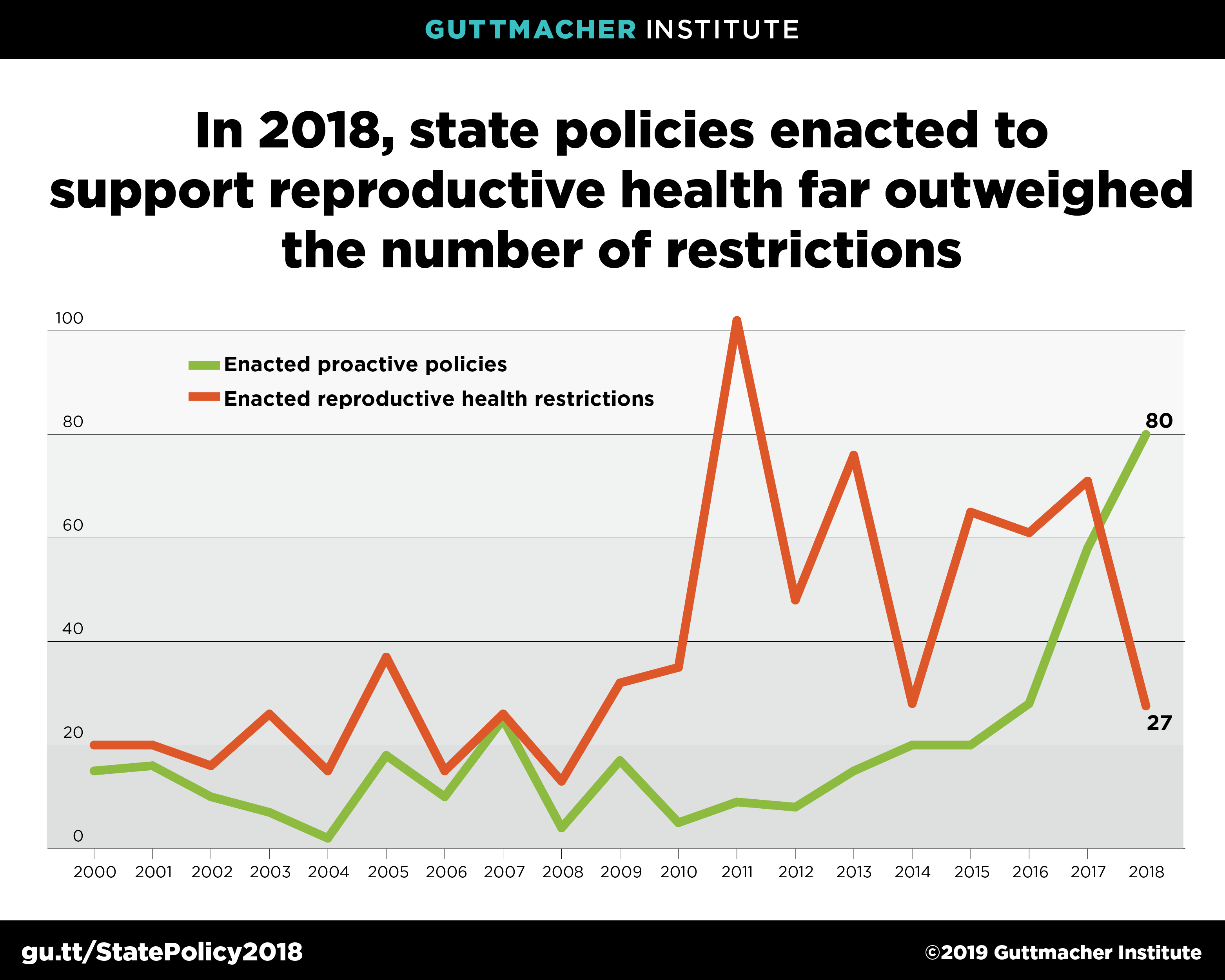
Over the course of 2018, 15 states adopted 27 new restrictions on abortion and family planning (see chart); 23 of these seek to restrict abortion and the remaining four are aimed at family planning providers. This marks the lowest number of new abortion restrictions enacted in at least a decade.
Perhaps even more significantly, 2018 was the first in recent years when the number of proactive policies enacted outpaced new restrictions. This year, 29 states and the District of Columbia enacted 80 measures that expanded access in the following categories: abortion and contraception, testing and treatment for STIs, reproductive health care for minors, infertility coverage and comprehensive sex education. These new proactive measures include five on abortion, 60 on contraception, 11 on sex education, three related to young people’s access to reproductive health care and one provision that allows expedited therapy for STIs. States also adopted an additional 40 measures in 2018 aimed at reducing maternal mortality or providing reproductive health services for incarcerated women.
Abortion
The 23 new abortion restrictions enacted in 2018 constitute the lowest number in a decade; in 2017, for example, states added 63 new restrictions. Although the new restrictions span a wide range of issue areas, bans on some abortions and new reporting requirements for abortion providers are two that showcase the ways states appear to be laying the groundwork for future litigation that would restrict abortion or abolish it entirely.
Abortion bans. Iowa’s ban is the most extreme antiabortion measure adopted this year; it would ban abortion at six weeks after the patient’s last menstrual period (LMP), based on the presence of a fetal heartbeat. Like a similar measure adopted by North Dakota in 2013, enforcement of the law was immediately blocked pending judicial review. Also this year, Louisiana and Mississippi adopted measures banning abortion at 15 weeks LMP. The Mississippi measure was challenged and in November, a federal district court struck down the ban. In an unusual approach to drafting legislation, the Louisiana law was written to go into effect only if the Mississippi law was implemented. Forty-three states have laws in effect that ban abortion at 20 weeks LMP or later, but none of the measures seeking to ban abortion earlier in pregnancy are in effect (see chart).

Both Kentucky and Ohio enacted measures to ban the most commonly used method of abortion in the second trimester—standard dilation and evacuation. The Kentucky ban was immediately blocked by legal action, the Ohio law is scheduled to take effect in March 2019. Mississippi and West Virginia have similar laws in effect, while comparable laws in six other states (Alabama, Arkansas, Kansas, Louisiana, Oklahoma and Texas) have been blocked (see Bans on Specific Abortion Methods Used After the First Trimester). As noted above, the case in Alabama has been appealed to the U.S. Supreme Court.
Reporting abortion complications. About half the states have long-standing requirements that abortion providers report to state agencies when complications occur (see Abortion Reporting Requirements). In 2018, three states (Arizona, Idaho and Indiana) enacted laws that go well beyond traditional reporting requirements. These laws greatly expand the scope of what is considered an abortion complication to include issues such as subsequent psychological or emotional problems, complications in subsequent pregnancies and later development of breast cancer. These provisions, which are not rooted in scientific evidence, appear to be part of a concerted effort by abortion opponents to build an evidence base to support their contention that abortion is dangerous.
Provisions to protect abortion rights or expand abortion access. Three states adopted five proactive measures related to abortion in 2018:
- Massachusetts repealed two long-standing abortion restrictions: the state’s pre-Roe abortion ban and a law requiring abortions after 13 weeks LMP to be performed in a hospital.
- Washington enacted a comprehensive reproductive health coverage law that requires private insurance coverage of abortion services in plans that also cover maternity care, with the same level of cost sharing as for maternity services.
- Louisiana adopted two measures: One exempts medication abortion from the requirements for the disposal of fetal tissue resulting from an abortion, and the other makes coercing someone into having an abortion a crime.
Unfortunately, California Gov. Jerry Brown vetoed a measure that would have required provision of medication abortion services on public college and university campuses.
Family Planning
States took a range of actions on issues related to family planning in 2018, some aimed at expanding coverage and access and others seeking to restrict it.
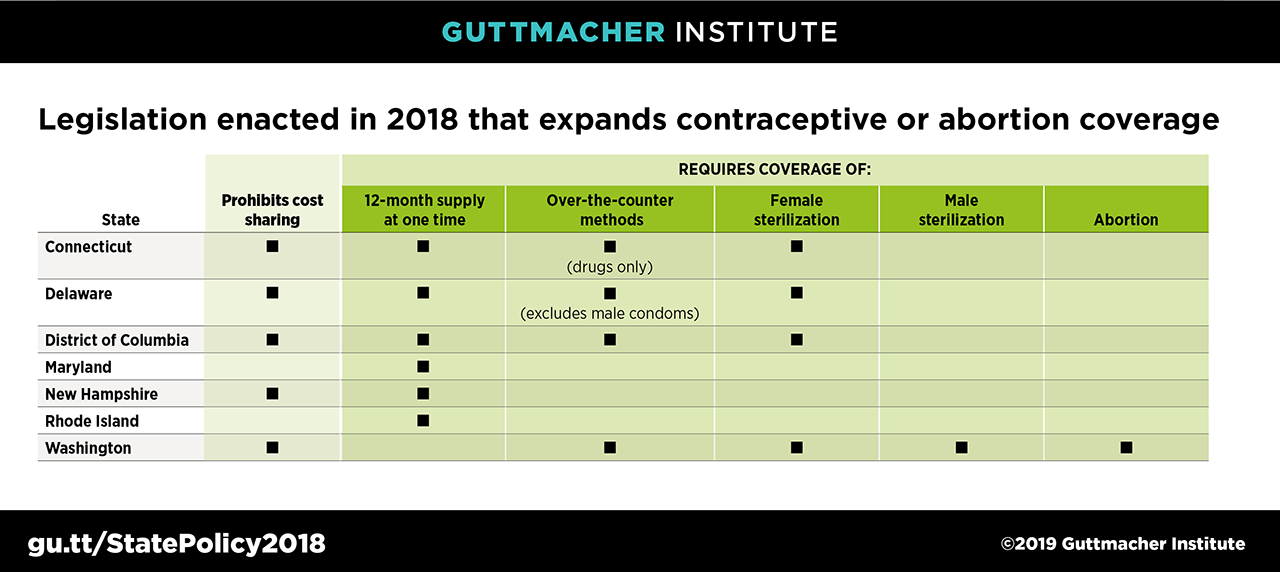
Coverage by private insurance. In the face of ongoing attempts by Congress and the Trump administration to restrict or repeal the Affordable Care Act, some states continued to shore up contraceptive coverage for their residents in 2018. Connecticut, Delaware, New Hampshire, Washington state and DC amended their existing contraceptive coverage guarantee to prohibit cost sharing by enrollees; when these measures go into effect in early 2019, 14 states will provide this coverage (see Insurance Coverage of Contraceptives). Connecticut, Delaware, New Hampshire, Rhode Island and DC moved to require insurers to cover a 12-month contraceptive supply at one time; Maryland extended the amount from a six-month to a 12-month supply. When these laws go into effect, 18 states and DC will require insurers to cover an extended supply of contraceptives at one time.
Publicly funded family planning. New Jersey and Utah both moved to expand Medicaid eligibility for individuals seeking family planning services. New Jersey is seeking federal permission to extend coverage to individuals with an income up to 200% of the federal poverty level ($12,140 for a single-person household and $20,780 for a family of three); currently, the eligibility ceiling is 138% of the poverty level for both parents and childless adults, according to the Kaiser Family Foundation. (The state also restored $7.5 million in family planning funds that had been cut by the previous governor, Chris Christie.) Utah is seeking to extend Medicaid eligibility for family planning services to individuals with incomes up to 95% of the poverty level; currently, parents in the state are eligible with incomes up to 60% of the poverty level and there is no coverage for childless adults. Along similar lines, Maryland is seeking to extend its current income eligibility ceiling from 200% to 250% of the poverty level. Virginia is seeking federal approval to make its current Medicaid family planning expansion permanent. Currently, 25 states have federal approval to extend Medicaid eligibility for family planning services to individuals who would otherwise not be eligible for full Medicaid insurance coverage based on their income (see Medicaid Family Planning Eligibility Expansions).
South Carolina and Tennessee both moved to prohibit Planned Parenthood from receiving reimbursements under their state Medicaid program, bringing the number of states to have attempted to exclude the organization from participating in Medicaid to 12; Arkansas is the only state where courts have allowed this restriction to go into effect (see State Family Planning Funding Restrictions). Louisiana rolled back a ban on the state contracting with any entity that had any financial relationship with Planned Parenthood; the exclusion had applied to Medicaid as well as any other state funds. Iowa rolled back a provision that would have barred hospitals that provide abortion from participating in its state-run family planning program; the program had been a joint federal-state Medicaid family planning expansion until 2017, when the state ended its partnership with the federal government in order to exclude Planned Parenthood and other organizations that provide abortion services.
Sex Education
Against the backdrop of heightened public attention to issues related to sexual harassment, several states moved in 2018 to revamp their requirements for sex education in schools. Six states (Colorado, Illinois, Georgia, Washington, West Virginia and Wyoming) added a requirement that sex education provided in the state include prevention of dating and sexual violence; this brings the number of states requiring coverage of these topics to 33, plus DC. Illinois, Maryland and Rhode Island added a requirement for coverage of consent issues in sex education classes; including these states, 5 states require a discussion of the importance of consent. Utah mandated that classes include a discussion of refusal skills, bringing the number of states requiring a discussion of this topic in sex or HIV/STI education to 24. Currently 28 states and DC mandate at least some sex education topics (see Sex and HIV Education).